
Журнал «Почки» Том 10, №2, 2021
Вернуться к номеру
Примусова гідратація при ХХН стадій 1–5: огляд і детальний аналіз трьох клінічних досліджень
Авторы: Mariia D. Ivanova(1), Anatoliy I. Gozhenko(2), Tommy Crestanello(3), Dmytro D. Ivanov(1)
(1) — Shupyk National Healthcarе University of Ukraine, Kyiv, Ukraine
(2) — Ukrainian Scientific Research Institute of Transport, Odesa, Ukraine
(3) — Milan, Italy
Рубрики: Нефрология
Разделы: Справочник специалиста
Версия для печати
Метою паралельного двогрупового проспективного багатоцентрового рандомізованого дослідження під назвою «HYD45 — Гідратація при 4–5-й стадіях ХХН», проведеного в 62 пацієнтів із ХХН G4–5, була оцінка розрахункової швидкості клубочкової фільтрації (рШКФ) із тренуванням для збільшення споживання води (CIWI) з досягненням мінімально вищого діурезу на 400 мл у 31 пацієнта порівняно з групою ХХН G4–5 без CIWI. Зазначена тривалість становила 12 місяців, але дослідження було припинене через 6 місяців через більш виражене зниження рШКФ у групі CIWI, а саме: –3,3 мл проти 2 мл у групі без CIWI. РШКФ, функціональний резерв нирок (ФНР), співвідношення альбуміну й креатиніну та якість життя пацієнта додатково проаналізовані в цьому дослідженні. Також було проаналізовано три рандомізованих клінічних дослідження, у яких пацієнти з хронічною хворобою нирок стадій 1–2, 3 та 4–5 отримували гідратацію. Результати досліджень вказують на можливу ефективність примусової гідратації на 1–2-й стадії ХХН, що спостерігається в пацієнтів із нормальним або підвищеним функціональним резервом нирок. На стадії 3 ХХН примусова гідратація не показала переваг, а на стадії 4–5 призвела до більшої втрати функції нирок. Узагальнюючи ці дані, автори дійшли висновку, що здоровим людям доцільно споживати кількість рідини, яка забезпечує фізіологічний діурез 1,2–1,8 л та нормоосмолярність сечі. CIWI часто виявляється надмірною, примусова надмірна гідратація може не сприяти здоровому способу життя. CIWI стає вимушеною надмірною гідратацією, оскільки функція нирок знижується. Можливо, переваги CIWI втрачаються при ХХН із прогресуванням втрати функції нирок. Вплив на рШКФ протягом 12 місяців може бути позитивним для ХХН стадії 1 та ХХН стадії 2 з нормальним функціональним нирковим резервом. CIWI, мабуть, недоцільна для хронічних, 3–5-ї, стадій. При ХХН стадії 4–5 ФНР втрачається, що, ймовірно, пояснює негативний вплив на рШКФ. При ХХН G1 CIWI призводить до оптимального збереження функції нирок зі збільшенням показника рШКФ на 1 мл/хв/1,73 м2 на рік порівняно з тим самим споживанням води. При ХХН G2 CIWI запобігає фізіологічній та патологічній втраті функції нирок, ФНР понад 50 % сприяє відновленню рШКФ при ХХН G1–2. Випробування ECIWIC демонструє переваги CIWI в пацієнтів із ХХН G1–2 зі збереженим ФНР, яке може бути рекомендоване для гальмування прогресування ХХН.
Параллельное в 2 группах проспективное многоцентровое рандомизированное исследование под названием «HYD45 — Гидратация при ХБП 4–5-й стадий», выполненное у 62 пациентов с ХБП G4–5, было направлено на оценку рСКФ при проведении принудительной гидратации (CIWI) с достижением более высокого диуреза минимально на 400 мл у 31 пациента по сравнению с группой из 31 пациента с ХБП G4–5 без CIWI. Заявленная продолжительность исследования составляла 12 месяцев, исследование было прекращено через 6 месяцев из-за более выраженного падения рСКФ в группе CIWI, а именно: –3,3 мл по сравнению с 2 мл в группе без CIWI. В этом исследовании дополнительно анализировались рСКФ, почечный функциональный резерв (ФПР), соотношение альбумина и креатинина и качество жизни пациента. Кроме того, были проанализированы три рандомизированных клинических исследования, в которых пациенты с ХБП стадий 1–2, 3 и 4–5 получали гидратацию. Результаты исследований указывают на возможную эффективность CIWI при 1–2-й стадии ХБП, которая встречается у пациентов с нормальным или повышенным функциональным резервом почек. На стадии 3 ХБП CIWI не показала положительных результатов, а на стадии 4–5 ХБП принудительная гидратация приводила к большей потере функции почек. Обобщая эти данные, авторы пришли к выводу, что здоровым людям, вероятно, целесообразно потреблять такое количество жидкости, которое обеспечивает физиологический диурез 1,2–1,8 л и нормоосмолярность мочи. CIWI часто бывает чрезмерной, принуждение к чрезмерной гидратации может не способствовать здоровому образу жизни. CIWI превращается в принудительную избыточную гидратацию по мере снижения функции почек. Возможно, преимущества CIWI теряются при ХБП с прогрессированием потери почечной функции. Положительный эффект CIWI в течение 12 месяцев может быть положительным при ХБП 1-й и 2-й стадии с нормальным функциональным резервом почек. CIWI, вероятно, нецелесообразна для хронических стадий 3–5. При ХБП 4–5 ФПР не сохраняется, что, вероятно, объясняет негативный эффект CIWI. При ХБП G1 CIWI приводит к сохранению функции почек с увеличением СКФ на 1 мл/мин/м2/год по сравнению с тем же потреблением воды. При ХБП G2 CIWI предотвращает физиологическую и патологическую потерю функции почек, ФПР выше 50 % способствует восстановлению рСКФ при ХБП G1-2. Исследование ECIWIC демонстрирует преимущества CIWI у пациентов с ХБП G1–2 и сохраненным ФПР и может быть рекомендовано для торможения прогрессирования ХБП.
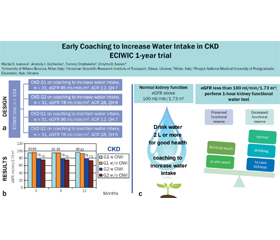
Parallel two-group prospective multicentre randomized trial named “HYD45 — Hydration in CKD 4–5 stages” that enrolled 62 patients with CKD G4–5 was aimed at evaluating of estimated glomerular filtration rate (eGFR) with coaching to increase water intake (CIWI) with the achievement of minimally higher diuresis by 400 mL in 31 patients compared with the CKD G4–5 group without CIWI. The stated duration was 12 months, and the trial was terminated in 6 months due to a more pronounced eGFR drop in the CIWI group, namely –3.3 ml vs. 2 ml in the group without CIWI. eGFR, renal functional reserve (RFR), albumin-to-creatinine ratio, and patient’s quality of life were additionally analyzed in this trial. Finally, three randomized clinical trials were analyzed in which patients with CKD 1–2, 3, and 4–5 received hydration. The results of studies demonstrate the possible efficacy of CIWI in stage 1–2 CKD in patients with normal or increased renal functional reserve. In stage 3 CKD, CIWI showed no benefits, and in stage CKD 4–5, forced hydration resulted in greater renal function loss. Summarizing these data, the authors concluded that it is probably appropriate for healthy people to consume the amount of fluid that provides physiological diuresis of 1.2–1.8 L and urine normal osmolarity. CIWI is often excessive, forced excessive hydration may not promote a healthy lifestyle. CIWI becomes forced excess hydration as kidney function decreases. Possibly, the benefits of CIWI are lost in CKD with the progression of renal function reduction. The effect of CIWI for 12 months may be positive for stage 1 CKD and stage 2 CKD with normal functional renal reserve. CIWI is probably impractical for chronic stages 3–5 CKD. In CKD 4–5, RFR is not preserved, which probably explains the negative effect of CIWI. With CKD G1, the CIWI leads to the optimal preservation of the renal function with the increase of GFR per 1 ml/min/1.73 m2 per year in comparison with the same water intake. In CKD G2, CIWI prevents physiological and pathological loss of renal function, RFR above 50 % provides restoration of eGFR in CKD G1–2. Early Coaching to Increase Water Intake in CKD (ECIWIC) trial demonstrates benefits of CIWI in patients with CKD G1–2 and preserved RFR and may be recommended to delay the CKD worsening.
раннє тренування для збільшення споживання води (примусова гідратація) при ХХН; розрахункова швидкість клубочкової фільтрації; функціональний нирковий резерв
ранняя тренировка по увеличению потребления воды (принудительная гидратация) при ХБП; расчетная скорость клубочковой фильтрации; функциональный резерв почек
early coaching to increase water intake in CKD; eGFR; renal functional reserve
Background
Materials and methods
Results and discussion
/9.jpg)
/9_2.jpg)
/10.jpg)