Вступ
Згинальна контрактура колінного суглоба (неповне розгинання гомілки) — патологічний стан, що негативно впливає на опорно-кінематичну функцію нижньої кінцівки й значно погіршує якість життя пацієнта.
Нормальний обсяг рухів у колінному суглобі має діапазон від 2–3° перерозгинання до 140–145° згинання згідно з нейтральним нуль-прохідним методом вимірювання й записується як (2/0/140)°. У людей з порушенням функції колінного суглоба знижується активний діапазон рухів через нездатність згиначів гомілки подовжуватися при розгинанні [1] до фізіологічної довжини. Ці порушення можуть бути тимчасовими, виникають з різних причин, різняться за ступенем вираженості й характером супутніх клінічних проявів.
Згинальна контрактура колінного суглоба в низці випадків може бути пов’язана із запальною реакцією на руйнування елементів суглоба, наприклад, при ревматоїдному артриті чи остеоартрозі [2], з порушенням біомеханіки або виникає при вроджених деформаціях. Іноді згинальна контрактура розвивається після операцій на колінному суглобі як наслідок тривалої іммобілізації чи рубцевих змін у покривних тканинах [3–6].
У хворих зі згинальними контрактурами внаслідок проєкційного вкорочення кінцівки помітно змінюється навантаження хворої кінцівки, що веде до порушення ходьби, збільшення навантаження на чотириголовий м’яз і зростання контактних напружень в пателофеморальному й кульшових суглобах. При цьому скорочується час опори через більш ранній відрив п’ятки від опорної поверхні, а при контрактурі понад 15° передній поштовх (або контакт п’ятки з опорною поверхнею) може взагалі бути відсутнім. При нормальному кроці стопа контактує з опорною поверхнею всією площиною, при значній контрактурі — тільки пальцями. У пацієнтів зменшується довжина кроку [7], з’являються іпсилатеральні нахили таза при опорі на хвору кінцівку, бічні й вертикальні розхитування тулуба, виражена кульгавість [1]. Біомеханічні порушення спостерігаються не тільки при ходьбі, але й при стоянні, через що для збереження вертикальної пози хворому необхідно прикладати більше зусиль, ніж зазвичай [8]. Вертикальна поза стає менш стійкою.
З часом згинальна контрактура колінного суглоба може призводити до формування згинальної конт-рактури іпсилатерального кульшового суглоба, що значно порушує просторову орієнтацію тіла при стоянні й ходьбі [9], рухи стають більш енергоємними, через що виникає м’язовий дисбаланс хребта й таза. Це, у свою чергу, знижує якість життя й обмежує функціональні можливості пацієнта, заважає особистому життю.
Зміна природних анатомічних співвідношень в одному суглобі веде до зміни навантаження в суміжних суглобах і провокує розвиток дегенеративних змін [2, 10–13]. При тривалому перебігу процесу (декілька років) порушуються не тільки біомеханіка ходьби, але й генетична програма руху, патологічна звичка перетворюється в набутий патологічний патерн [14].
Мета роботи: на моделі ходьби вивчити роботу м’язів нижньої кінцівки за умови контрактури колінного суглоба різного ступеня вираженості. Визначити мінімально необхідну силу м’язів нижньої кінцівки для здійснення нормального кроку.
Матеріали та методи
Аналіз ходи проводили в програмі OpenSim 4.0 [15]. За основу моделювання взято модель gait2394 [16, 17], що дозволяє вивчати 76 м’язів нижніх кінцівок і тулуба. Немасштабована модель є об’єктом зі зростом 1,8 м і масою 75,16 кг.
Досліджували порушення роботи м’язів при контрактурах колінного суглоба, які моделювали шляхом обмеження розгинання стегна на 10°, 15° і 20°. Аналіз проводили для м’язів правої нижньої кінцівки, порівнюючи отримані показники з показниками базової моделі (тієї ж кінцівки без обмеження розгинання).
Вивчали роботу тільки тих м’язів, що забезпечують згинання-розгинання гомілки в колінному суглобі:
— задня група — згиначі гомілки (також беруть участь у розгинанні стегна): m. biceps femoris — двоголовий м’яз стегна (окремо довга й коротка головка), m. semimembranosus — напівперетинчастий м’яз, m. semi-
tendinosus — напівсухожильний м’яз; лише литкова порція триголового м’яза гомілки m. gastrocnemius;
— медіальна група — згинач гомілки — m. gracilis — тонкий м’яз;
— передня група м’язів стегна: m. sartorius — кравецький м’яз — згинач стегна й гомілки, а також m. quadriceps femoris — чотириголовий м’яз стегна (окремо rectus, vastus medialis і сумарно vastus intemedius et lateralis) — розгинач гомілки й згинач стегна.
Аналіз зміни сили м’язів нижньої кінцівки проводили відносно часових параметрів кроку. За основу взята 8-фазна модель ходи [18], тому що вона найбільш повно описує:
1. Передній поштовх (0,65 с) — перший період опорної фази кроку, коли п’ята торкається опорної поверхні. Стегна в положенні легкого згинання, гомілка повністю розігнута в колінному суглобі (фаза двохопорного стояння).
2. Фаза перекату з п’яти на стопу (0,65–0,83 c) — у цій фазі в навантаження послідовно включаються спочатку п’ята, потім уся стопа. Стегно поступово розгинається, гомілка поступово згинається від 0° до 15° у колінному суглобі.
3. Фаза перекату зі стопи на передній відділ (0,83–0,87 c) — у цій фазі руху центр тяжкості тіла знаходиться під стопою, протилежна кінцівка не торкається опорної поверхні (період одноопорного стояння). Стегно поступово розгинається, гомілка поступово розгинається від 15° флексії до 0° (до нейтрального положення) у колінному суглобі.
4. Задній поштовх (0,87–1,15 c) — п’ята відривається від поверхні, навантаження перерозподіляється на головки плеснових кісток. Стегна повністю розігнуті, гомілка в положенні від нейтрального (0°) до повного розгинання (3–5° перерозгинання в колінному суглобі).
5. Фаза відриву опорної кінцівки від площини опори (1,15–1,27 c) — розгинання стегна зменшується, гомілка поступово згинається до 30–35° у колінному суглобі, пальці стопи відриваються від поверхні.
6. Початок фази перенесення (1,27–1,48 с) — стегно поступово згинається, гомілка прогресивно згинається в колінному суглобі до 60°.
7. Середня фаза перенесення (1,48–1,63 с) — стегно згинається за рахунок скорочення м’язів передньої поверхні стегна, гомілка з положення згинання в 60° прогресивно розгинається до нейтрального положення (0°) у колінному суглобі. У цій фазі вага тіла повністю розподілена на протилежну ногу.
8. Остаточна фаза перенесення (1,63–1,8 с) — максимальне згинання стегна до 30°, повне розгинання гомілки (до 3–5° перерозгинання в колінному суглобі), стопа займає нейтральне положення.
Результати
У роботі досліджували роботу м’язів при контрактурах колінного суглоба, які моделювали шляхом обмеження розгинання стегна на 10°, 15° і 20°. Аналіз проводили для м’язів правої нижньої кінцівки, порівнюючи з показниками базової моделі для тієї ж кінцівки без обмеження рухів.
Вивчали роботу тільки м’язів, які відповідальні за згинання-розгинання гомілки в колінному суглобі.
Аналіз зміни сили м’язів нижньої кінцівки проводили відносно часових параметрів кроку. За основу взята 8-фазна модель ходьби [15].
Цикл ходьби описують 8 подіями [7] (рис. 1).
Початковий контакт (0 % циклу ходьби) відповідає початку опори, коли п’ятка вперше торкається поверхні.
Реакція на навантаження (10 % циклу ходьби) виникає, коли контралатеральна стопа відривається від поверхні.
Відрив п’ятки (30 % циклу ходьби) відповідає відриву п’ятки від поверхні.
Протилежний початковий контакт (50 % циклу ходьби) відповідає контакту стопи протилежної кінцівки с поверхнею.
Відрив носка стопи (60 % циклу ходьби) — носок стопи опорної кінцівки відривається від поверхні.
Суміщення стоп (73 % циклу ходьби) — період, коли стопа махової кінцівки знаходиться на одній осьовій лінії зі стопою опорної.
Вертикальна стегнова кістка (87 % циклу ходьби) відповідає моменту, коли стегнова кістка махової ноги орієнтована вертикально.
Остання подія є початковим контактом, який фактично є початком наступного циклу ходьби.
Ці вісім подій ділять цикл ходьби на сім періодів.
Реакція на навантаження — період між початковим контактом і відривом носка стопи протилежної кінцівки, вагу тіла приймає опорна кінцівка (від 0 до 10 % циклу ходьби).
Середня стойка — від відриву носка стопи протилежної кінцівки до початку підйому п’ятки (від 10 до 30 % циклу ходьби).
Кінцева стойка починається з моменту підйому п’ятки й закінчується, коли протилежна кінцівка торкається поверхні (від 30 до 50 % циклу ходьби).
Передмах — від контакту стопи протилежної кінцівки до відриву носка іпсилатеральної стопи, що за часом відповідає другому періоду двохопорної стойки (від 50 до 60 % циклу ходьби).
Початок маху — від відриву стопи до моменту суміжних стоп (від 60 до 73 % циклу ходьби).
Середина маху — від суміжних стоп до позиції вертикального положення стегнової кістки махової ноги (від 73 до 87 % циклу ходьби).
Завершення маху — від вертикального положення стегнової кістки до контакту п’ятки (від 87 до 100 % циклу ходьби).
Завдання, які виконуються під час циклів
Перші 10 % циклу ходьби відповідають завданню прийняття ваги, коли маса тіла передається з однієї кінцівки на протилежну.
Одноопорна підтримка (від 10 до 50 % циклу ходьби) — кінцівка, яка навантажена, приймає на себе вагу тіла, а протилежна виконує мах.
За даними моделювання, контрактура колінного суглоба в першу чергу впливає на функцію підколінних сухожилків м’язів задньої групи стегна (згиначів гомілки), до яких відносять m. biceps femoris, m. semitendinosus і m. semimembranosus.
M. biceps femoris (двоголовий м’яз стегна) — м’яз задньої поверхні стегна, він складається з двох голівок — довгої (biceps femoris — long head) і короткої (biceps femoris — short head). M. biceps femoris — коротка головка — єдиний м’яз, що відповідає за функцію згинання колінного суглоба [19]. Робота м’яза в умовах обмеження рухів у колінному суглобі подана на рис. 2.
/20.jpg)
Аналіз отриманих результатів моделювання показав, що зі збільшенням ступеня обмеження рухомості колінного суглоба збільшується необхідне для виконання кроку скорочення м’язів. Особливо це помітно у фазах заднього поштовху, відриву стопи від поверхні й на початку переносу стопи (від 1,0 с до 1,4 с), при цьому колінний суглоб максимально розгинається. При контрактурах 10° і 15° необхідно значне збільшення зусилля м’язів в цих фазах кроку, але при контрактурі 20° м’яз практично не бере участі в цих фазах руху. При контрактурі 15° і 20° пік скорочення m. biceps femoris — коротка головка припадає на початок фази відриву пальців (1,35–1,37 с), тобто на момент, коли м’яз повинен виконувати свою безпосередню роботу — починати згинати гомілку для переносу стопи. У нормі при контрактурі 10° скорочення м’язів виражене помірно.
М’язи задньої поверхні стегна m. semitendinosus, m. semimembranosus і m. biceps femoris — довга головка крім роботи зі згинання колінного суглоба виконують функцію згинання й приведення стегна. Їх робота за умови контрактури колінного суглоба наведена на рис. 3
M. semitendinosus и m. semimembranosus беруть початок від сідничного бугра й закінчуються у верхній частині медіальної поверхні великогомілкової кістки й у ділянці медіального виростка великогомілкової кістки.
M. biceps femoris — довга головка починається також від сідничного бугра, іде до верхньої головки малогомілкової кістки, тобто за наявності контрактури в колінному суглобі ці м’язи змінюють кут дії сили застосування.
Результати моделювання показали, що сила скорочення m. semimembranosus збільшується у 2,5 раза у фазі переднього (0,65 с) і заднього (1,86 с) поштовхів, тобто в моменти максимального розгинання колінного суглоба. Аналогічно виглядає робота m. semitendinosus, але скорочення в ці ж фази у 5–7 разів більші. При контрактурі 20° можна спостерігати практично відсутність роботи mm. semimembranosus і semitendinosus через контрактильний стан.
Робота m. biceps femoris — довга головка виглядає дещо по-іншому. При контрактурі 10° зміни в роботі незначні, але при контрактурах у 15° і 20° спостерігається значне збільшення сили скорочення починаючи з моменту опори на стопу (1,0 с) і до відриву пальців (1,5 с), тобто у фазі перекату стопи на її передній відділ, під час якого відбувається максимальне розгинання коліна.
За згинання колінного суглоба відповідальні м’язи gracilis і sartorius, які здійснюють також згинання стегна. M. gracilis бере участь у приведені, а m. sartorius — у відведені стегна. Робота цих м’язів за умови контрактури колінного суглоба наведена на рис. 4.
M. gracilis проходить практично вертикально від нижньої сіднично-лобкової гілки до медіальної поверхні великогомілкової кістки, тому дуже чутливий навіть до незначних змін кута дії сили, що й показано на рис. 4а. Якщо при контрактурі 10° зміни в роботі спостерігаються тільки в момент переднього поштовху (0,65 і 1,86 с), то при контрактурах 15° і 20° скорочення м’яза спостерігається в усіх фазах кроку, особливо у фазі переносу стопи (з 1,4 с до 1,6 с), причому скорочення збільшується зі збільшенням кута контрактури.
M. sartorius — тонкий довгий поверхневий м’яз передньої поверхні стегна, що проходить від передньої верхньої клубової кістки через кульшовий і колінний суглоби до медіальної поверхні великогомілкової кістки. Отже, м’яз бере участь в стабілізації таза, кульшового й колінного суглоба. Як показують результати моделювання, найбільш перевантажений цей м’яз у фазі відриву пальців стопи й на початку фази переносу стопи (1,15–1,4 с).
За згинання колінного суглоба й плантарне згинання стопи відповідають м’язи medial і lateral gastrocnemius — м’язи задньої поверхні гомілки. М’язи беруть початок від капсули колінного суглоба й косої підколінної зв’язки й ідуть до п’яткової кістки, займаючи всю задню поверхню гомілки [2]. Від якості їх роботи залежить також функціональність стопи (рис. 5), плавність перекату стопи, ритмічність ходьби.
Як показали результати моделювання, більш сильний м’яз m. medial gastrocnemius при збільшенні конт-рактури зменшує свою силу. У нормі м’яз має два моменти скорочення — на 1,0 с (фаза відриву п’ятки) і 1,2 с (фаза відриву пальців стопи), у цей період колінний суглоб максимально розігнутий. При контрактурі 10° зменшується сила скорочення на 1,0 с, при контрактурі 15° період скорочення м’яза розтягується до 1,3 с, тобто займає всю фазу перекату стопи. При 20° відбувається обмеження рухів, сила м’яза значно зменшена при опорі на стопу, але вимоги до сили збільшуються при розгинанні гомілки в остаточній фазі переносу стопи і фазі переднього поштовху (1,75 с).
M. lateral gastrocnemius у нормі має один пік скорочення на 1,05–1,35 с, що відповідає фазі перекату стопи на передній відділ, при контрактурах скорочення м’яза розтягується на весь одноопорний період кроку.
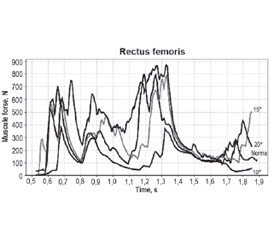
M. quadriceps femoris (чотириголовий м’яз) — найбільший м’яз тіла людини [20]. Він складається з чотирьох порцій, які ми розглядаємо окремо: три порції m. vastus lateralis (великий латеральний м’яз), m. vastus medialis (медіальний широкий м’яз стегна), m. vastus intermedius (проміжний широкий м’яз стегна) відповідають за розгинання колінного суглоба, а прямий м’яз стегна (m. rectus femoris) — додатково за згинання стегна. Vastus medialis, intemedius, lateralis працюють симетрично з незначним перевищенням сили латеральної порції, тому зручно аналізувати м’язи сумарно (рис. 6).
Зміни в роботі m. rectus femoris при збільшенні ступеня контрактури добре показані на рис. 6, сила скорочення м’яза у фазі перекату стопи на передній відділ збільшується в 3 рази, а при 20° переходить у стан постійного скорочення, тільки в період переносу стопи із зігнутим коліном (1,5–1,7 с) спостерігається зниження активності м’яза практично до нормального.
В аналогічному стані перебуває широкий м’яз стегна. Якщо при контрактурі 10° зміни в роботі незначні, то вже при 15° спостерігаються піки скорочення як при опорі на стопу, так і при переносі стопи, а при 20° контрактури м’яз перебуває в стані скорочення постійно. Це пояснюється тим, що м’язи намагаються розігнути колінний суглоб у необхідні фази кроку, але їх сили недостатньо для виконання цієї функції.
Обговорення
За отриманими результатами моделювання можна зробити такі висновки. Контрактура колінного суглоба не тільки порушує функцію самого суглоба, але й патологічно впливає на функцію кульшового й гомілкового суглобів через універсальність роботи більшості двосуглобових м’язів стегна й гомілки.
При контрактурах колінного суглоба найбільше страждають розгиначі гомілки. Це пояснюється тим, що для забезпечення правильної ходьби необхідне повноцінне розгинання гомілки і цим м’язам необхідно розвивати силу, яка здатна подолати контрактуру. Наприклад, при контрактурі 20° для розгинання колінного суглоба модель повинна розвивати силу 2250 Н, але в реальності, за даними Delp (1990) [17], максимально можлива ізометрична сила становить 780 Н, що майже в 3 рази менше.
Одним з м’язів, які найбільше впливають на функціональність кульшового суглоба, є m. semitendinosus. У нормі сила, яку він розвиває при ходьбі, становить близько 90 Н, тоді як при контрактурах необхідна сила збільшується до 200 Н, і хоча цей м’яз здатен розвивати силу до 330 Н, у наших моделях простежується його явне надмірне скорочення.
Значно порушується робота m. gracilis і m. sartorius. У нормі їх сила не перевищує 20 Н, а при обмеженні рухливості колінного суглоба необхідна сила збільшується в 4 й більше рази — до 90–110 Н, тобто м’яз працює на межі своїх можливостей (105–110 Н).
Із перевищенням своїх функціональних можливостей при контрактурах колінного суглоба працює m. biceps femoris — коротка головка. Максимальна сила скорочення, яку здатен розвивати цей м’яз, становить 400 Н, тоді як у моделях з контрактурами колінного суглоба необхідне для нормальної ходьби зусилля сягає 900 Н, що, звісно, м’яз у реальних умовах розвивати не може.
Висновки
Контрактура колінного суглоба призводить до зміни біомеханіки всієї нижньої кінцівки. Обмеження рухливості колінного суглоба веде до наростання змін у роботі м’язів, змушуючи їх працювати в умовах постійної напруги або, навпаки, виключаючи їх з роботи, що призводить до різкого порушення ходи. Знаючи вплив контрактури колінного суглоба на роботу м’язів нижньої кінцівки, можна прогнозувати перебіг патологічного процесу, визначити, які групи м’язів страждають найбільше. Враховуючи особливості їх функціонування при тому чи іншому ступені обмеження рухливості колінного суглоба, можна визначити, яка група м’язів потребує корекції до і після оперативного втручання.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів і власної фінансової зацікавленості при підготовці даної статті.
Отримано/Received 25.04.2022
Рецензовано/Revised 09.05.2022
Прийнято до друку/Accepted 18.05.2022
Список литературы
1. Klatt J., Stevens P.M. Guided growth for fixed knee flexion deformity. J. Pediatr. Orthop. 2008. 28(6). 626-31. doi: 10.1097/BPO.0b013e318183d573. PMID: 18724198.
2. Netter F. Atlas of Human Anatomy. 6th Edition. Elsevier Saunders; 2014.
3. Карпинский М.Ю., Карпинская Е.Д., Щикота Р.А., Тяжелов А.А., Гончарова Л.Д. Результаты моделирования повреждений связочного аппарата коленного сустава. Травма. 2012. 13(3). 165-171.
4. Пустовойт К.Б., Карпінський М.Ю. Моделювання умов навантаження колінного суглоба з позицій механіки. Клінічна хірургія. 2013. 53-56. EID: 2-s2.0-84878858969.
5. Damsin J.P., Ghanem I. Treatment of severe flexion deformity of the knee in children and adolescents using the Ilizarov technique. J. Bone Joint Surg. Br. 1996. 78(1). 140-4. PMID: 8898146.
6. Grishkevich V.M., Vishnevsky A.V. Postburn Knee Flexions Contractures: Anatomy and Methods of Their Treatment. Trop. Med. Surg. 2013. 1. 6. doi: 10.4172/2329-9088.1000147.
7. Jankovic J., Albanese A., Atassi M.Z., Dolly J.O., Hallett M., Mayer N.H. Botulinum Toxin E-Book: Therapeutic Clinical Practice and Science, Philadelphia, Saunders Elsevier; 1997.
8. Filipenko V., Arutunan Z., Mezentsev V., Tankut O., Karpinska O., Karpinsky M. Stratographic measurements in patients after total knee replacement. Orthopaedics, Traumatology and Prosthetics. 2019. 4. 12-17. doi: 10.15674/0030-59872019412-17.
9. Harato K., Nagura T., Matsumoto H., Otani T., Toyama Y., Suda Y. A gait analysis of simulated knee flexion contracture to elucidate knee-spine syndrome. Gait Posture. 2008. 28(4). 687-92. doi: 10.1016/j.gaitpost.2008.05.008.
10. Chapman G.J., Halstead J., Redmond A.C. Comparability of off the shelf foot orthoses in the redistribution of forces in midfoot osteoarthritis patients. Gait Posture. 2016. 49. 235-240. doi: 10.1016/j. gaitpost.2016.07.012.
12. Levinger P., Menz H.B., Morrow A.D. Foot kinematics in people with medial compartment knee osteoarthritis. Journal of Foot and Ankle Research. 2011. 4(1). doi: 10.1186/1757- 1146-4-S1-O27.
13. Rzaniak E., Dzierzanowski M., Matewski D. Wpływ zmian zwyrodnieniowych stawów biodrowych na ukształtowanie stopy. Kwartalnik Ortopedyczny. 2007. 3. 342-351.
14. Tyazhelov O., Karpinsky M., Karpinska O., Branitsky O., Obeidat Khaled. Pathological postural patterns at condition of long-term joint osteoarthritis of the lower extremity. Orthopaedics, Traumatology and Prosthetics. 2020. 1. 26-31. doi: http://dx.doi.org/10.15674/0030-59872020126-32.
15. Delp S.L., Anderson F.C., Arnold A.S., Loan P., Habib A., John C.T., Guendelman E., Thelen D.G. OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 2007. 54(11). 1940-50. doi: 10.1109/TBME.2007.901024.
16. Anderson F.C., Pandy M.G. Dynamic optimization of human walking. Journal of Biomechanical Engineering. 2001. 123. 381-390
17. Delp S.L., Loan J.P., Hoy M.G., Zajac F.E., Topp E.L., Rosen J.M. An interactive graphics-based model of the lower extremity to study orthopaedic surgical procedures. IEEE Transactions on Biomedical Engineering. 1990. 37. 757-767.
18. Loudon J., Bell S., Johnston J.M. The clinical orthopedic assessment guide. Kansas: Human Kinetics, 2008. 395-408.
19. Su E.P. Fixed flexion deformity and total knee arthroplasty. J. Bone Joint Surg. Br. 2012. 94 (11 Suppl. A). 112-5. PMID: 23118396.
20. Bordoni B., Varacallo M. Anatomy, Bony Pelvis and Lower Limb, Thigh Quadriceps Muscle. StatPearls [Internet]. Last Update: February 7, 2021.

/19.jpg)
/20_2.jpg)
/21.jpg)
/21_2.jpg)
/22.jpg)