Резюме
Мета дослідження: вивчити структуру й особливості динаміки первинної інвалідності серед дорослого населення України в результаті неонкологічних урологічних захворювань за формуючими її хворобами. Матеріали та методи. Використано форму звітності № 14 Держкомстату України, статистичні збірники ДУ «Український державний НДІ медико-соціальних проблем інвалідності» й документацію регіональних медико-соціальних експертних комісій. Результати. Виявлено тенденцію до зменшення кількості осіб, уперше визнаних інвалідами внаслідок хвороб сечостатевої системи (ССС). Підтверджено, що цьому сприяє продовження тимчасової втрати працездатності. Офіційна звітність щодо причин інвалідності за класом хвороб ССС стосується лише хронічного гломерулонефриту й хронічного пієлонефриту: за 5 років частка першої нозології збільшилася на 13,0 % (до 43,8 % серед 1549 зареєстрованих), другої — зменшилася на 37,4 % (до 20,0 % у всіх регіонах, крім м. Києва). Одночасно спостерігалася тенденція до зменшення частки виходу на інвалідність з причин, віднесених до «інших» (36,2 ± 2,0 % проти 39,0 ± 1,8 % у 2016 р., а в Центральному і Північно-Східному регіонах — 49,2 ± 2,8 % і 49,6 ± 4,7 % відповідно). За винятком двох вищезгаданих патологій, структура причин інвалідності така: перші три місця посідали сечокам’яна хвороба (СКХ), полікістоз, єдина нирка, наступні три — гідронефроз, уроджені вади й стриктура сечівника. З віком збільшується частота випадків при СКХ, полікістозі, гідронефрозі, стриктурі сечівника й зменшується — при уроджених вадах і єдиній нирці. З роками зменшується також частка призначення ІІ групи інвалідності (18,1 ± 3,1 % у 2020 р. проти 20,4 ± 2,6 % у 2016 р.) і відбувається збільшення частки ІІІ групи (67,8 ± 3,8 % проти 65,3 ± 3,1 %) при стабільних показниках I групи (14,1 проти 14,3 %). Висновки. За 5-річний період спостереження на 12,9 % більше пацієнтів уникли інвалідності і на 4,7 % менше отримали І і ІІ групу. Зменшення частки хронічного пієлонефриту як причини інвалідності на 37,4 % (до 20,0 %) спостерігалось у всіх регіонах, окрім м. Києва. Структура інших причин інвалідності: сечокам’яна хвороба — 45,0 %, полікістоз нирок — 22,1 %, єдина нирка — 18,8 %, гідронефроз — 15,4 %, уроджені вади — 12,1 %, стриктура сечівника — 4,7 %. На тлі загального зростання призначень інвалідності з віком частіше призначалася інвалідність ІІІ групи (7,7 % — до 39 років, 63,1 % — у передпенсійному віці, 67,8 % — у пенсійному).
Background. The purpose of the work: to study the structure and features of the dynamics of primary disability among the adult population of Ukraine as a result of non-oncological urological diseases. Materials and methods. The reporting form No. 14 of the State Statistics Service of Ukraine, the statistical sources of the Ukrainian State Research Institute of Medical and Social Problems of Disability, documentation of regional centers for medical and social expertise are used. Results. There is a tendency to reduce the number of people recognized as disabled for the first time due to genitourinary diseases. It has been confirmed that prolonging temporary disability contributes to this. The official reporting of the causes of disability by the class of genitourinary diseases is presented only for chronic glomerulonephritis and chronic pyelonephritis; for 5 years, the incidence of the first nosology increased by 13.0 % (to 43.8 % among 1,549 registered), the second — decreased by 37.4 % (to 20.0 % in all regions except Kyiv). At the same time, there was a tendency to reduce the incidence of disability retirement for reasons classified as “others” (36.2 ± 2.0 % vs. 39.0 ± 1.8 % in 2016, and in the Central and Northeastern regions it reached 49.2 ± 2.8 % and 49.6 ± 4.7 %, respectively). Apart from the two above-mentioned pathologies, the structure of disability causes is as follows: the first three places belonged to urolithiasis, polycystic kidney disease, single kidney, the next three — hydronephrosis, congenital malformations and urethral stricture. With age, the incidence of urolithiasis, polycystic kidney disease, hydronephrosis, urethral stricture increases and the incidence of congenital malformations and a single kidney decreases. Over the years, the assignment of the second group of disability decreases (18.1 ± 3.1 % in 2020 vs. 20.4 ± 2.6 % in 2016), with an increase of the third group (67.8 ± 3.8 % vs. 65.3 ± 3.1 %), and stabilization of the first group (14.1 vs. 14.3 %). Conclusions. During the 5-year observation period, 12.9 % more patients avoided disability and 4.7 % less received groups I and II. A decrease by 37.4 % (to 20.0 %) in the share of chronic pyelonephritis as a cause of disability was observed in all regions except Kyiv. Structure of other causes of disability: urolithiasis — 45.0 %, polycystic kidney disease — 22.1 %, single kidney — 18.8 %, hydronephrosis — 15.4 %, congenital defects — 12.1 %, urethral stricture — 4.7 %. Against the background of the general increase in disability assignments with age, group III disability among others was more common (7.7 % — at the age of up to 39 years, 63.1 % — at pre-retirement age, 67.8 % — at retirement age).
Introduction
Public health, according to the World Health Organization, is a set of organizational measures aimed at preventing disease and prolonging human life. Investments in health cover a wide range of costs for prevention, payment for medical services, rehabilitation [1–4]. A separate, relevant area is the management of people with disabilities who are among the most active users of medical care in outpatient clinics and hospitals and need social services. The World Health Organization emphasizes the prevalence of disability over the years, along with the growing elderly and senile population and the consequent reduction in healthy life expectancy with significant economic damage. No country can avoid it. Therefore, the formation of social and economic policy in each of them is determined not only by the degree of understanding the problem, but also the development of the health care system and by socio-economic situation [5, 6].
The predominance of people with disability groups III (55 %) and II indicates untreated patients who were referred to the medical and social expert commissions (MSEC) by doctors from medical control commissions. Hence the importance of coordinated work of medical and social examination and outpatient services in the rehabilitation of patients with chronic debilitating diseases. At present, the practice of medical and social expertise, the principles of classification and criteria for establishing disability, types of medical and social care need to be improved [7]. Reorganization of medical care aimed at prevention, early diagnosis, post-hospital therapy with rehabilitation in outpatient and sanatorium conditions, adaptation at the social level are the main principles for solving disability problems [8–10]. The above justifies the need to study the regional dynamics of the causes of disability, in this case due to genitourinary diseases.
Purpose: to study the structure and features of the dynamics of primary disability due to non-oncological urological diseases among the adult population of Ukraine.
Materials and methods
Several sources of information are used in the work. The first was the reporting form No. 14 “Report on the causes of disability, indications for medical, professional and social rehabilitation”, approved by the Order of the Ministry of Health of Ukraine No. 378 dated 10.07.2007 by agreement with the State Statistics Service of Ukraine (chapter 4 “Distribution of people newly diagnosed with a disability by disease classes and individual nosological forms”, chapter 5 “Of the total number of people newly diagnosed with a disability”). The class of genitourinary diseases in the document is represented by only two nosological forms: chronic glomerulonephritis and chronic pyelonephritis [11, 12]. The statistical sources of the Ukrainian State Research Institute of Medical and Social Problems of Disability of the Ministry of Health of Ukraine were selected as the second source of information [13, 14].
On a contract basis, the materials of the following regional MSECs were also used: Ivano-Frankivsk, Ternopil (Western region), Cherkasy (Central), Sumy (Northeast), Dnipropetrovsk (Southeast), Mykolaiv, Odesa, Kherson (South). The total adult population of these areas in 2020 was 10,066,417 people of both sexes, which was 29.4 % of the total population of Ukraine (34,198,849). Among them, 27.9 % (6,662,304) were urban residents (23,883,921) and 33.0 % (3,404,113) — rural (10,314,928).
The indicators of 2020 and 2016 were analyzed and compared: absolute values and calculated intensive, extensive coefficients, average values and mean errors. The latter was used to determine Student’s criterion for assessing the significance of the differences between the two statistical coefficients.
Results and discussion
The issue of disability of people of working age due to non-oncological urological diseases, despite its relevance, was last discussed in the literature available to us in 1991 [15, 16]. The analysis of the current state of the problem showed that in Ukraine, the total number of people disabled due to genitourinary diseases is reducing over the years. Thus, in 2020, 1,549 people were recognized as disabled for the first time, which was 13.0 % less than in the previous year (1,782) and 13.7 % for five consecutive years (1,795). Moreover, in 2016–2020, the process affected all regions: in the West — by 5.1 % to 479, in the Center — by 8.8 % to 301, in the Northeast — by 2.3 % to 115, in the Southeast — by 23.3 % to 385, in the South — by 12.0 % to 162 and in Kyiv — by 13.0 % to 108 people. In 2016, the most cases occurred in the Western and Southeastern regions (505 and 502 people), they shared the first place (28.1 ± 1.6 % and 28.0 ± 1.0 %, respectively). The second was Central region, where 18.4 ± 0.9 % (330) was concentrated, the third was Southern — 10.2 ± 0.2 % (184), followed by Northeastern (8.4 ± 0.6 %) and the capital (6.9 ± 0.6 %). In 2020, the distribution remained the same, but with an increase in the share of the contingent in the Western region and its decrease in the Southeast (to 31.0 ± 1.3 % and 24.9 ± 1.0 %, respectively), i.e. it became clearer. At the same time, it is worth pointing out the significant fluctuations in the number of people recognized as disabled for the first time in some administrative territories. According to their number, Kyiv and four regions (Lviv, Dnipropetrovsk, Kharkiv, Odesa) attracted attention in 2016, with the exception of Kharkiv region in 2020. They accounted for 39.2 ± 1.1 % and 36.5 ± 1.2 %, respectively, i.e. 704 of 1,795 and 566 of 1,549 people (p < 0.05).
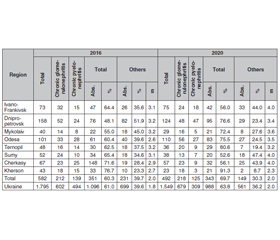
It has been confirmed that in addition to effective inpatient treatment with subsequent rehabilitation in outpatient settings (outpatient-polyclinic, sanatorium, etc.), one of the most important and effective means for preventing disability is the extension of sick leaves through MSEC. In recent years, this principle of treating patients with urological diseases has become more common and sophisticated, as shown in Table 1.
/56.jpg)
So, if in 2016 there were 49 such cases and this number is taken as 100 %, then with each year they increased by 36.7, 16.3, 4.1 %, and in 2020 by 51.0 % (74 people). The share of patients who completed treatment in each current year is also growing, namely by 41.2, 11.8, 20.6 and 94.1 % according to the value of the coefficient, provided that 34 cases in 2016 are accepted as 100 %. This nature of change indicates the feasibility of the existing approach. At present, more patients have returned to active life and daily work without restrictions and have not been considered disabled. The share of such people over the years was 73.5, 54.2, 55.3, 63.4 and 86.4 %, respectively, for 2016–2020. It is worth noting that most people considered disabled were assigned group III. In particular, in 2016, there were 9 of 34 such patients after completion of treatment (26.5 %), in subsequent years, 19 of 48 (39.6 %), 17 of 38 (44.7 %), 12 of 41 (29.3 %) and 8 of 66 (12.1 %), respectively. Meanwhile, 3 people received group I–II in 2017 (6.2 %), 3 (7.3 %) in 2019 and 1 (1.5 %) in 2020.
Probably, the fact that the share of primary disability due to genitourinary diseases in Ukraine for many years is low (in 2016 and 2020, it was 1.4 and 1.5 and 1.3 and 1.4 %, respectively, for the adult and working-age population, or 0.6 and 0.7 and 0.5 and 0.6 per 10 thousand), explains the special shortage of available statistics on certain nosological forms. Information is limited to chronic glomerulonephritis and chronic pyelonephritis. In 2016, they accounted for 33.5 ± 1.9 % and 27.5 ± 2.0 %, respectively, in Ukraine as a whole. Over 5 years, the share of chronic glomerulonephritis has significantly increased and the share of chronic pyelonephritis has decreased (in 2020, 43.8 ± 1.9 % and 20.0 ± 2.2 %, respectively). An increase in chronic glomerulonephritis is due to an increase in cases in the West (from 31.5 ± 1.9 % to 49.7 ± 2.2 %; p < 0.05), Southeast (from 35.2 ± 2.1 % to 41.6 ± 2.5 %; p < 0.05), South (from 35.3 ± 3.5 % to 55.6 ± 3.9 %; p < 0.05) and in the capital (from 13.7 ± 3.0 % to 45.4 ± 4.7 %, p < 0.05). In the other two regions, the nature of the changes was reversed. At the same time, the proportion of chronic pyelonephritis has decreased significantly in all regions except Kyiv. The data hidden under “other reasons” are of particular interest. Their share with a declining trend remains high across the country (from 39.0 ± 1.8 % in 2016 to 36.2 ± 2.0 % in 2020). At the same time, in the Central and Northeastern regions, the indicator reaches almost 50 % (49.2 ± 2.8 % and 49.6 ± 4.7 % vs. 39.7 ± 2.6 % and 33.3 ± 3.8 % in 2016; p < 0.05). This prompted to expand the study with the results of the MSEC operational data of eight regions, with an emphasis on detailing and clarifying other reasons.
Table 2 shows that the number of people recognized as disabled for the first time in the defined territory was 582 in 2016, 492 in 2020, i.e. 32.4 and 31.8 % of their number in Ukraine, respectively. Involvement of more than a third of cases testifies to the representativeness of the sample. Proof of this is the preservation of the general sign of disability reduction (for 5 years by 15.5 %). In addition, the same nature of changes in indicators can be seen in all observations, as well as their close values. In particular, the percentage of chronic glomerulonephritis as a cause of disability is growing (36.4 ± 1.9 % and 44.3 ± 2.2 % in 2016 and 2020, respectively; p < 0.05), it is lower, but still remains high among “others” (39.7 ± 2.0 % and 30.3 ± 2.0 %; p < 0.05). The incidence of chronic pyelonephritis remains similar (23.9 ± 1.7 % and 25.4 ± 1.9 % vs. 27.5 ± 2.0 % and 20.0 ± 2.2 % in Ukraine as a whole in 2016 and 2020, respectively). This situation is quite acceptable given its course and prevalence both as an independent disease, and as a complication of almost all infectious and inflammatory diseases.
The results of the study on the causes of primary disability among the adult population of Ukraine due to urological pathology depending on age and nosology (except for chronic pyelonephritis) according to MSEC materials of eight regions are presented in Table 3. It was found that urolithiasis occupies a leading position. However, its share decreased significantly, from 45.0 ± 3.2 % in 2016 to 26.8 ± 3.6 % in 2020; p < 0.05. The age-specific feature of disability of patients with urolithiasis has been established. It was manifested by a decrease in the number of people under 39 years, those of pre-retirement and retirement age, but significantly in the first two categories (39.5 ± 4.7 % vs. 19.6 ± 6.2 %, 47.5 ± 4.8 % vs. 31.0 ± 6.2 % and 55.6 ± 4.8 % vs. 50.0 ± 6.2 %, respectively).
/57.jpg)
There were significantly fewer patients whose disability was due to nephrectomy (7.4 ± 2.1 % in 2020 vs. 24.2 ± 2.8 % in 2016) and the results of surgery (3.3 ± 1.4 % vs. 6.9 ± 1.6 %, respectively). This should be considered a consequence of achievements in the diagnosis, treatment and metaphylaxis of the disease. However, the presence of stones in both kidneys tends to increase among the causes of disability (from 13.9 ± 2.2 % to 16.1 ± 3.0 %).
The second place in the structure of the causes of disability is occupied by polycystic kidney disease with a tendency to increase over the years: in 2016 — 19.0 ± 2.5 %, in 2020 — 22.1 ± 3.3 % (p > 0.05). There is an increase in such cases among the younger population. Thus, if in 2016 the above three age categories accounted for 16.0 ± 5.5 %, 19.8 ± 6.0 % and 33.3 ± 7.0 %, then in 2020, 19.6 ± 7.0 %, 23.8 ± 7.4 % and 25.0 ± 7.5 %, respectively. Given the nature of the course of polycystic kidney disease, this can be explained by its late detection in the stage of decompensation.
Third place in 2020 belonged to a single kidney as a cause of disability, which accounted for significantly more cases than in 2016: 18.8 ± 3.2 % vs. 8.7 ± 1.8 % (five years after, this place belonged to congenital malformations — 17.7 ± 2.5 %). It is noteworthy that the number of patients with a single kidney as a cause of disability decreases with age: from 21.3 % under the age of 39 to 17.8 % at the age of 40–55 and 40–60 years among women and men, respectively. The reverse nature of changes against the background of significantly lower indicators was observed in 2016, namely: 7.4, 10.0 and 11.1 %, respectively, for three age periods.
As for birth defects, they lost their third place in 2016, taking fifth place in 2020. Their share was 17.7 ± 2.5 % vs. 12.1 ± 2.6 %; p < 0.05. However, twice as many cases with age are a common feature for them: in 2016, 28.4 and 12.1 % among people under 39 and 40–55 and 40–60 years (women, men), and in 2020, 16.4 and 9.5 %, respectively. This confirms the latent nature of the course, and hence the untimely detection of pathology with such adverse consequences.
Hydronephrosis was the most common cause of disability. It ranks fourth in 2020 and fifth in 2016 (15.4 ± 2.9 % and 6.5 ± 1.6 %, respectively; p < 0.05). Urethral stricture among the causes of disability consistently occupies the last sixth place, its share was 4.7 ± 1.7 % and 3.0 ± 1.1 % in 2020 and 2016, respectively. The multifactorial etiology, duration and complexity of treating patients explain an increase in such cases with age and years of follow-up (from 3.3 to 6.0 %, respectively, in people under 39 and at pre-retirement age in 2020, while in 2016, 2.5 and 3.5 %, respectively).
Over the years, the share of cases of group II disability decreases (18.1 ± 3.1 % in 2020 vs. 20.4 ± 2.6 % in 2016; p > 0.05), there is a tendency to increase the figure with group III (67.8 ± 3.8 % vs. 65.3 ± 3.1 %, respectively) with stabilization of the frequency of assignment of group I (14.1 vs. 14.3 %, respectively). There is also an age dependence in the form of a less frequent assignment of group III, more frequent — of group II and even more clearly — of group I.
If in 2016 rural residents predominated (52.4 ± 4.5 % vs. 47.6 ± 4.7 % of urban residents; p > 0.05), then in 2020, on the contrary, there were 53.7 ± 5.5 % of urban residents vs. 46.3 ± 6.0 % of rural (p > 0.05). In addition, patients of pre-retirement age dominated in rural areas (97.5 vs. 94.5 % in urban areas), while in 2020, the situation has changed — among urban residents, younger people dominated (97.5 vs. 94.2 %).
The distribution by sex has also differed. In 2016, males who were recognized as disabled for the first time prevailed significantly, namely 58.3 ± 3.2 % vs. 41.7 ± 3.2 % of females; in 2020, the difference between the indicators decreased to 53.6 ± 4.1 % and 46.4 ±4.0 %, respectively (p > 0.05).
Conclusions
1. The effective application of the approach of extended sick leaves led to a 51.0% increase in the number of patients who complete treatment in each current year, which, in turn, allowed 12.9 % more patients to avoid disability and 4.7 % less (only 1.5 vs. 6.2 % in 2017) — to be assigned group I–II.
2. According to official reports, chronic glomerulonephritis and chronic pyelonephritis together accounted for 1,096 of 1,795 cases (61.0 %) in 2016, and 988 of 1,549 (63.8 %) in 2020. A decrease in the share of chronic pyelonephritis as a cause of disability by 37.4 % (to 20.0 %) was observed in all regions except Kyiv.
3. According to the results of a nested sampling from 8 regions of Ukraine, 582 and 492 people were recognized as disabled for the first time due to diseases of the urinary and male reproductive systems, which accounted for 32.4 and 31.7 % of their total number in Ukraine in 2016 and 2020, respectively. The following structure of disability causes was determined (with the exception of chronic glomerulonephritis and chronic pyelonephritis): urolithiasis — 45.0 % in 2020 vs. 26.8 % in 2016; polycystic kidney disease — 22.1 vs. 19.0 %; single kidney — 18.8 vs. 8.7 %; hydronephrosis — 15.4 vs. 6.5 %; congenital defects — 12.1 vs. 17.7 %; urethral stricture — 4.7 vs. 3.0 %, respectively.
4. The general feature of an increase in the number of patients recognized as disabled for the first time in the following pathologies was established: urolithiasis — 19.6 % under 39 years, 31.0 % at pre-retirement age, 50.0 % at retirement age; polycystic kidney disease — 19.6, 23.8, 25.0 %, respectively; hydronephrosis — 19.6 % under the age of 39 and 25.0 % at pre-retirement age; urethral strictures — 3.3 and 6.0 %, respectively. A decrease was noted for congenital defects — from 16.4 to 9.5 % in those under 39 years and at pre-retirement age; single kidney — from 21.3 to 17.8 %, respectively.
5. Over the years, a decrease was noted in the assignments of disability group II (18.1 % in 2020 vs. 20.4 % in 2016), an increase in group III (67.8 vs. 65.3 %), with stabilization of group I (14.1 vs. 14.3 %). At the same time, it was found that group III was assigned more frequently with age (7.7 % — up to 39 years old, 63.1 % — at pre-retirement age, 67.8 % — at retirement age), the number of group II assignments increased (14.3, 28.2 and 25.0 %, respectively) and even more clearly — of group I (8.2, 16.7 and 30.0 %, respectively).
Received 19.07.2022
Revised 02.08.2022
Accepted 10.08.2022

/56.jpg)
/57.jpg)