Резюме
Актуальність. Проблема вибору об’єму операцій на щитоподібній залозі (ЩЗ) з приводу однобічного вузлового зоба з компресійним синдромом гостро стоїть перед хірургами. У таких випадках хірургічне лікування є абсолютно показаним. При цьому можливими варіантами об’єму операції є тиреоїдектомія і гемітиреоїдектомія. Тиреоїдектомія дозволяє ліквідувати вогнище автоімунної агресії в організмі, але в таких випадках пацієнт приречений пожиттєво вживати препарати тироксину. Мета роботи: визначення показань до вибору об’єму операції у хворих на однобічний вузловий зоб з компресійним синдромом на тлі автоімунного тиреоїдиту (АІТ) і прогнозування віддалених результатів хірургічного лікування. Матеріали та методи. Проаналізовані віддалені результати гемітиреоїдектомії у 101 жінки віком від 23 до 72 років, хворої на однобічний вузловий зоб з компресійним синдромом на фоні АІТ (ВЗАІТ). Провели аналіз, за яких об’єму частки залози, варіанта ехоструктури, рівнів у крові ТТГ, вільних тироксину і трийодтироніну, антитіл до ТПО, показників апоптозу і проліферації до операції відзначалися задовільні і незадовільні результати лікування. Результати. Задовільний результат відзначався у 75 хворих (перша група), у яких, за даними обстеження, через 3 роки після гемітиреоїдектомії не виявлено порушень функціонального стану ЩЗ, а, за даними УЗД, у паренхімі залишеної частки залози наявні до операції ознаки АІТ не прогресували або ж прогресували без розвитку гіпотиреозу і зміни варіанта ехографічної картини. Другу групу (незадовільний результат) становили 26 хворих, у яких через 3 роки після гемітиреоїдектомії, за даними УЗД, встановлено збільшення об’єму залишеної частки ЩЗ та прогресування автоімунного процесу з розвитком гіпотиреозу. На задовільний результат гемітиреоїдектомії у лікуванні хворих на ВЗАІТ із компресійним синдромом можна розраховувати у випадках, коли на момент операції об’єм частки становить не більше 12,7 см3, її ехоструктура відповідає гіпоехогенному і гетерогенному та псевдомікровузловому варіантам, ТТГ не вище за 2,85 мМО/л, рівні вільних тироксину і трийодтироніну відповідно не нижче за 16,7 та 5,3 пмоль/л, показник АТ-ТПО не вище за 137 МО/мл. Висновки. Одним із можливих варіантів хірургічного лікування хворих на ВЗАІТ з компресійним синдромом може бути гемітиреоїдектомія за умов збереженої гормональної функції залози з помірно вираженими процесами проліферації та апоптозу і структурних змін паренхіми на рівні гіпоехогенного і гетерогенного, псевдомікровузлового ехоструктурних варіантів. Вважаємо протипоказаним застосовування гемітиреоїдектомії у випадках псевдовеликовузлового і більших за тяжкістю варіантів ехоструктури паренхіми щитоподібної залози незалежно від показників гормонопродукуючої функції, АТ-ТПО, проліферації та апоптозу.
Background. The problem of choosing the extent of surgeries on the thyroid gland for unilateral nodular goiter with compression syndrome is of concern for surgeons. In such cases, surgical treatment is absolutely indicated, and the possible variants of the extent of the operation are thyroidectomy and hemithyroidectomy. Thyroidectomy allows eliminating the focus of autoimmune aggression in the body, but in such cases, a patient should use thyroxine drugs for life. The purpose was to determine the indications for the choice of the extent of surgery in patients with unilateral nodular goiter and compression syndrome against the background of autoimmune thyroiditis (AIT) and to predict long-term results of surgical treatment. Materials and methods. The long-term outcomes of hemithyroidectomy were analyzed in 101 women aged 23 to 72 years with unilateral nodular goiter on the background of AIT and compression syndrome. We have analyzed the volume of the gland, echostructure variant, blood levels of thyroid-stimulating hormone (TSH), free thyroxine and triiodothyronine, thyroid peroxidase (TPO) antibodies, apoptosis and proliferation indicators before surgery in which treatment results were satisfactory and unsatisfactory. Results. Satisfactory result was revealed is 75 patients (group 1). According to the survey, they had no violations of the thyroid functional state 3 years after hemithyroidectomy, and, according to the ultrasound, in the parenchyma of the remaining lobe of the gland, the signs of AIT present before the surgery did not progress or progressed without hypothyroidism and changed ultrasound picture. The second group (unsatisfactory result) consisted of 26 patients who 3 years after hemithyroidectomy had an increase in the volume of the remaining thyroid gland and the progression of autoimmune process with the development of hypothyroidism on ultrasound. A satisfactory result of hemithyroidectomy in patients with unilateral nodular goiter on the background of AIT with compression syndrome can be expected in cases where at the time of surgery, the volume of the lobe is not more than 12.7 cm3, the echostructure is hypoechoic, heterogeneous and pseudomicronodular, TSH is not more than 2.85 mIU/l, levels of free thyroxine and triiodothyronine are not lower than 16.7 and 5.3 pmol/l, respectively, TPO antibodies are not higher than 137 IU/ml. Conclusions. One of the possible options for surgical treatment of patients with unilateral nodular goiter on the background of AIT with compression syndrome may be hemithyroidectomy in conditions of preserved hormonal function of the gland with moderate processes of proliferation and apoptosis, structural changes in the parenchyma at the level of hypoechoic and heterogeneous, pseudomicronodular echostructural variants. We consider it contraindicated to use hemithyroidectomy in cases of pseudomacronodular and more severe variants of the echostructure of the thyroid parenchyma, regardless of the indicators of hormone-producing function, TPO antibodies, proliferation and apoptosis.
Вступ
Проблема вибору об’єму операцій на щитоподібній залозі (ЩЗ) з приводу однобічного вузлового зоба з компресійним синдромом гостро стоїть перед хірургами. У таких випадках хірургічне лікування є абсолютно показаним. При цьому можливими варіантами об’єму операції є тиреоїдектомія і гемітиреоїдектомія. Тиреоїдектомія дозволяє ліквідувати вогнище автоімунної агресії в організмі, але в таких випадках пацієнт приречений пожиттєво вживати препарати тироксину. Гемітиреоїдектомія за умови збереженої гормонопродукуючої функції залишеної частки залози дозволить уберегти хворого від необґрунтованої тиреоїдектомії і пожиттєвої замісної терапії препаратами тиреоїдних гормонів [1].
Спрощений підхід до вибору об’єму операції, який базується переважно на даних УЗД, залишається чи не основною причиною виконання необґрунтованих за об’ємом хірургічних втручань. Діагностика вузлоутворення на тлі автоімунного тиреоїдиту (АІТ) становить певні труднощі, які зумовлені специфічними морфологічними і структурними змінами в тканині ЩЗ [2].
Морфологічну оцінку вузла до операції можна отримати лише за допомогою тонкоголкової аспіраційної пункційної біопсії (ТАПБ). Вважається, що точність цитологічної діагностики з допомогою ТАПБ становить близько 96,0–98,0 %. Проте на тлі АІТ точність морфологічної діагностики вузлових утворень знижується десь на 25,0 % і відповідно збільшується кількість сумнівних результатів [3]. У таких випадках підвищує точність цитологічної діагностики послідовне проведення цитоморфологічного й імуноцитохімічного досліджень на одному й тому ж мазку пункційного матеріалу [4].
Важливою ланкою діагностики є встановлення розладів регуляції клітинного циклу, зокрема проліферації і апоптозу. До їх маркерів відносять мембранні рецептори Fas і Fas-L, білки Bcl-2, ядерний генний супресор фосфопротеїн р53 та антиген Кі-67 [5–8]. Як свідчать дані літератури, включення цих маркерів у діагностичний комплекс дозволяє з високою точністю оцінювати та інтерпретувати вираженість і тяжкість автоімунних процесів у тканині ЩЗ. На нашу думку, ці показники можна застосувати для вибору об’єму хірургічного лікування при однобічному вузловому зобі на тлі АІТ з компресійним синдромом — гемітиреоїдектомії чи тиреоїдектомії.
Мета роботи: визначення показань до вибору об’єму операції у хворих на однобічний вузловий зоб з компресійним синдромом на тлі автоімунного тиреоїдиту і прогнозування віддалених результатів хірургічного лікування.
Матеріали та методи
Проаналізовані віддалені результати гемітиреоїдектомії у 101 жінки віком від 23 до 72 років, хворої на однобічний вузловий зоб з компресійним синдромом на тлі АІТ (ВЗАІТ). Тривалість захворювання на АІТ становила від 7 до 22 років. Діагноз встановлювали за даними клінічної симптоматики, результатами ультразвукового, лабораторних, морфологічних та імуногістохімічних досліджень. Клінічно звертали увагу на місцеві і загальні прояви АІТ. За даними УЗД вивчали структуру і кровопостачання ЩЗ, наявність, структуру, об’єм і локалізацію псевдо- і справжніх вузлових утворень та зміщення органів шиї.
За результатами УЗД, згідно з класифікацією Г.Дж. Бескін і співавторів (2018), у дослідження включали хворих лише з першими трьома варіантами ехографічної картини: гіпоехогенним і гетерогенним, псевдомікровузловим та псевдовеликовузловим [9]. З гіпоехогенним і гетерогенним варіантом була 51 хвора, з псевдомікровузловим — 27 і з псевдовеликовузловим — 23.
Визначали рівні тиреотропного гормону (ТТГ), вільних тироксину (вТ4), трийодтироніну (вТ3), антитіл до тиреоїдної пероксидази (АТ-ТПО). Досліджували пунктати з вузлового утворення та паренхіми протилежної частки. У пунктатах з вузла визначали його морфологічну характеристику за класифікацією The Bethesda system for reporting thyroid cytopathology, а в пункційному матеріалі з паренхіми залози протилежної частки вивчали активність автоімунного процесу за показниками проліферації і апоптозу. При приготуванні мазків ТАПБ використовували розроблений в Інституті ендокринології та обміну речовин ім. В.П. Комісаренка НАМН України і запатентований метод відновлення активності антигенних детермінант, який дозволяє поєднати цитоморфологічні та імуноцитохімічні дослідження на одному цитологічному препараті і надає можливість об’єктивної характеристики окремих клітинних елементів [4]. Результати імуногістохімічних реакцій оцінювали методом напівкількісного аналізу, який розроблений О.К. Хмельницьким [10]. Імунореактивні клітини вираховували за формулою: ІІРК (Fas, FasL, Bcl-2, р53) = N1/N2 × 100 %, де N1 — число клітин, імунопозитивних до Fas, FasL, Bcl-2, р53 рецепторів, N2 — загальне число ядер клітин на одному квадратному міліметрі. Оцінку ІПА здійснювали за формулою: ІПА = NKi-67/N заг. × 100 %, де NKi-67 — загальна кількість ядер, імунопозитивних до білка Ki-67, N заг. — загальна кількість ядер клітин на одному квадратному міліметрі. Для морфометричних досліджень використовували мікроскоп Bresser Bio Science Bino (Німеччина) з цифровою камерою «Нікон DS-Філь» та персональний комп’ютер з встановленим програмним забезпеченням NIS-Elements F 3.2.
При плануванні можливості виконання гемітиреоїдектомії у хворих на ВЗАІТ з компресійним синдромом брали до уваги результати ультрасонографії (ехоструктура, об’єм залози і частки без вузла), показники гормональної функції ЩЗ і АТ-ТПО, маркерів апоптозу та проліферації, дані цитологічних досліджень.
Усім хворим виконана операція гемітиреоїдектомія за загальноприйнятою методикою. Під час операції проводили гістологічне експрес-дослідження вузлових утворень. Розбіжностей результатів гістологічного експрес-дослідження та дослідження пункційного матеріалу не було.
Віддалені результати хірургічного лікування (гемітиреоїдектомії) оцінювали через три роки після операції за клінічними даними, результатами УЗД (розміри, ехоструктура і об’єм залишеної частки залози), показниками рівнів гормонів (ТТГ, вТ4, вТ3), АТ-ТПО, активності процесів проліферації та апоптозу. Вивчали, при яких досліджуваних показниках на момент включення пацієнтів у програму дослідження після хірургічного лікування відзначалося прогресування АІТ у залишеній частці залози з розвитком гіпотиреозу, що спричинило незадовільний результат лікування.
Комісією з біоетики Тернопільського національного медичного університету імені І.Я. Горбачевського Міністерства охорони здоров’я України засвідчено відповідність проведених досліджень морально-етичним нормам (протокол № 58 від 29 квітня 2020 року).
Статистичну обробку отриманих результатів дослідження проводили за допомогою електронних таблиць Microsoft® Office Excel та програмою для статистичного обчислення BioStat. Критичний рівень значущості (р) при перевірці статистичних гіпотез у даному дослідженні приймали рівним 0,05.
Результати
За віддаленими результатами хірургічного лікування однобічного вузлового зоба з компресійним синдромом на тлі АІТ виділили дві групи обстежених хворих.
Пацієнти першої групи (задовільний результат) — це 75 хворих, у яких через 3 роки після гемітиреоїдектомії визначався еутиреоз, а, за даними УЗД, у паренхімі залишеної частки залози наявні до операції ознаки АІТ не прогресували або ж прогресували без розвитку гіпотиреозу і зміни варіанта ехоструктури паренхіми залози.
Другу групу (незадовільний результат) становили 26 хворих, у яких через 3 роки після гемітиреоїдектомії визначався гіпотиреоз, а також, за даними УЗД, встановлено погіршення ехоструктури залишеної частки ЩЗ у межах одного ехоструктурного варіанта або ж з розвитком більш тяжкого варіанта. У трьох випадках прогресування автоімунного процесу супроводжувалось зміною ехоструктурного варіанта з псевдовеликовузлового на виражено гіпоехогенний (табл. 1). Для компенсації гіпотиреозу хворі отримували замісну терапію препаратами тироксину в дозах від 50 до 150 мкг на добу.
Дані, наведені в табл. 1, свідчать про те, що при гіпоехогенному і гетерогенному варіанті ехоструктурної картини в ЩЗ не було незадовільних результатів лікування. У разі псевдомікровузлового варіанта у 6 (22,2 %) випадках із 27 встановлений незадовільний результат лікування, який проявлявся прогресуванням АІТ і розвитком гіпотиреозу. Подібна клінічна ситуація спостерігалася у 17 (73,9 %) із 23 хворих з псевдовеликовузловим варіантом УЗ-змін у ЩЗ.
Проведені дослідження дозволили встановити, що в групі хворих із задовільним результатом об’єм залишеної частки залози вірогідно не відрізнявся від початкових показників, а її функція визначалась у межах еутиреозу. У випадках із незадовільним результатом у 18 із 26 хворих об’єм частки залози збільшився на 15–47 % порівняно з початковими даними. Показники рівня гормонів на необхідній дозі замісної терапії перебували у межах референтних значень. Рівень АТ-ТПО в обох групах хворих був підвищеним. Лише у разі незадовільних результатів він був вірогідно вищим, ніж у групі хворих із задовільним результатом лікування (табл. 2).
/27.jpg)
Порівняльна оцінка показників маркерів проліферації та апоптозу до операції між групами із задовільним і незадовільним результатами лікування показала пригнічення активності апоптотичних процесів на тлі вираженої активації процесів проліферації. У пацієнтів з незадовільним результатом процес проявлявся вірогідно вищими показниками ІПА Ki-67, ІІРК FasL, ІІРК Bcl-2 та нижчими — ІІРК Fas і ІІРК p53. Ці дані дозволяють вважати, що у пацієнтів цієї групи впродовж терміну спостереження після хірургічного лікування прогресували проліферативні процеси в тиреоїдній паренхімі, які спричинили погіршення ехоструктури залози і розвиток гіпотиреозу (табл. 3).
Наступним етапом дослідження було встановлення взаємозв’язку між віддаленими результатами лікування, варіантами ехоструктури паренхіми залози, показниками гормональної функції, АТ-ТПО, проліферації та апоптозу (табл. 4, 5).
Обговорення
Отримані результати проведеного порівняльного аналізу досліджуваних показників при задовільних і незадовільних результатах лікування вказують на те, що з погіршенням ехоструктури залози її гормонопродукуюча функція знижується, підвищується рівень АТ-ТПО, зростає активність проліферативних процесів і пригнічується апоптоз.
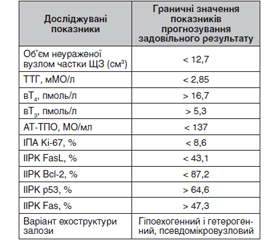
Результати проведених досліджень дають підстави пропонувати орієнтовні показники об’єму ЩЗ, її функції, АТ-ТПО, активності процесів проліферації і апоптозу, варіантів ехоструктури залози для вибору операції гемітиреоїдектомії і прогнозування задовільних наслідків лікування (табл. 6).
Розглядаючи псевдомікровузловий варіант ехоструктури, слід відзначити, що при цьому варіанті було 6 (22,2 %) хворих з незадовільним результатом лікування у випадках, коли об’єм частки без вузла перевищував 13,5 см3, АТ-ТПО — понад 150 МО/мл, ТТГ визначався на рівні понад 3 мМО/л, активність ІПА Ki-67 та ІІРК Bcl-2 була більшою і становила відповідно 10,5 та 89,1 %, а ІІРК p53 — менше ніж 60,2 %.
Отже, при виборі операції гемітиреоїдектомії при цьому варіанті ехоструктурних змін у частці залози потрібно особливу увагу звертати на показники об’єму частки, рівнів ТТГ та АТ-ТПО, активності процесів проліферації та апоптозу. При встановленні невідповідності значенням рекомендованих показників слід виконувати тиреоїдектомію.
Проведені дослідження вказують на те, що застосовані нами показники для вибору об’єму операції дозволяють розмежувати показання до тиреоїдектомії чи гемітиреоїдектомії у хірургічному лікуванні хворих на ВЗАІТ з компресійним синдромом.
Разом з цим вважаємо за доцільне наголосити на тому, що висновки цієї роботи базуються на результатах короткотривалих спостережень і не можуть бути рекомендовані для широкого впровадження в клінічну практику.
Висновки
Одним із можливих варіантів хірургічного лікування хворих на ВЗАІТ з компресійним синдромом може бути гемітиреоїдектомія за умов збереженої гормональної функції залози з помірно вираженими процесами проліферації та апоптозу і структурних змін паренхіми на рівні гіпоехогенного і гетерогенного та псевдомікровузлового ехоструктурних варіантів.
Вважаємо протипоказаним застосовування гемітиреоїдектомії у випадках псевдовеликовузлового і більших за тяжкістю варіантів ехоструктури паренхіми щитоподібної залози незалежно від показників гормонопродукуючої функції, АТ-ТПО, проліферації та апоптозу.
Етичне схвалення. Усі процедури проведеного дослідження із залученням пацієнтів відповідали етичним стандартам керівництв з клінічної практики та вимогам Гельсінської декларації (1964) з поправками. Пацієнти або юридичні опікуни пацієнтів підписали форми інформованої згоди на лікування та проведення всіх необхідних діагностичних процедур.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів та власної фінансової зацікавленості при підготовці даної статті.
Внесок авторів у роботу над статтею. Шідловський В.О. — дизайн, методологія, обробка матеріалу, написання та редагування тексту; Шідловський О.В. — обстеження хворих; Шеремет М.І., Лазарук О.В. — обробка матеріалу, написання та редагування тексту.
Отримано/Received 23.06.2022
Рецензовано/Revised 10.08.2022
Прийнято до друку/Accepted 02.09.2022

/27.jpg)
/28.jpg)
/28_2.jpg)