
Журнал «Медицина неотложных состояний» Том 19, №2, 2023
Вернуться к номеру
Градаційне дозування місцевого анестетика для проведення спінальної анестезії при ортопедо-травматологічних операціях на нижніх кінцівках
Авторы: Козловська І.Ю.
Вінницький національний медичний університет ім. М.І. Пирогова, м. Вінниця, Україна
Рубрики: Медицина неотложных состояний
Разделы: Клинические исследования
Версия для печати
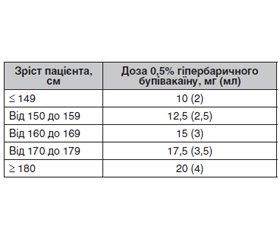
Актуальність. Розробка чіткого алгоритму дозування місцевого анестетика при проведенні спінальної анестезії під час операцій на нижніх кінцівках є актуальним питанням, навіть після століття використання цього методу знеболювання. Метою нашого дослідження є підвищення ефективності та безпеки спінальної анестезії під час оперативних втручань на нижніх кінцівках у пацієнтів ортопедичного та травматологічного профілю шляхом розробки алгоритму дозування місцевого анестетика. Матеріали та методи. Проведене дослідження ґрунтується на аналізі методик білатеральної спінальної анестезії у 75 хворих І–ІІ ступеня операційного ризику за ASA під час ортопедо-травматологічних операцій на нижніх кінцівках, розділених на 3 групи. Спінальна анестезія виконувалася спінальною формою 0,5% бупівакаїну за розробленим нами алгоритмом дозування анестетика відповідно до зросту пацієнта (3-тя група) та із стандартним рекомендованим дозуванням (1-ша група, пацієнти низького зросту, та 2-га група, зріст пацієнтів > 180 см). Результати. При дослідженні показників гемодинаміки під час оперативного втручання було встановлено, що частота серцевих скорочень (ЧСС) у хворих до початку операції становила: в 1-й групі — 73 ± 8 уд/хв, у 2-й групі — 78 ± 6 уд/хв, у 3-й групі — 79,32 ± 14,47 уд/хв. Через 30 хв після введення анестетика ЧСС у 1-й групі становила 68 ± 5 уд/хв, через 3 год після введення анестетика — 71 ± 9 уд/хв. У 2-й групі ЧСС у хворих через 30 хв після введення анестетика становила 79 ± 7 уд/хв, через 3 год після введення анестетика — 84 ± 9 уд/хв. У 3-й групі ЧСС у хворих через 30 хв після введення анестетика становила 71,56 ± 14,14 уд/хв, через 3 год після введення анестетика — 71,280 ± 9,002 уд/хв. Дані систолічного артеріального тиску (САТ) у хворих до початку операції: у 1-й групі — 139,6 ± 12,3 мм рт.ст., у 2-й групі — 136,0 ± 9,6 мм рт.ст., у 3-й групі — 138,40 ± 16,18 мм рт.ст. Протягом оперативного втручання показники артеріального тиску в 1-й групі становили: через 30 хв після введення анестетика — 113,0 ± 7,1 мм рт.ст., через 3 год після введення анестетика — 122 ± 14 мм рт.ст.; у 2-й групі: через 30 хв після введення анестетика — 138,0 ± 10,2 мм рт.ст., через 3 год після введення анестетика — 141,0 ± 12,5 мм рт.ст.; у 3-й групі: через 30 хв після введення анестетика — 102,48 ± 13,47 мм рт.ст., через 3 год після введення анестетика — 118,2 ± 10,0 мм рт.ст. Середня тривалість сенсорного блока у пацієнтів 1-ї групи становила 182,5 ± 17,2 хв, моторного блока — 130,0 ± 24,8 хв, у пацієнтів 2-ї групи сенсорний блок тривав 70,6 ± 13,1 хв, а моторний блок — 23,3 ± 6,7 хв, у пацієнтів 3-ї групи тривалість сенсорного блока становила 252,20 ± 74,32 хв та моторного блока — 198,2 ± 59,0 хв. Висновки. 1. Застосування малих доз гіпербаричного бупівакаїну не порушує гемодинамічні показники, але зменшує якість та тривалість анестезії у пацієнтів високого зросту. 2. Частота виникнення ускладнень під час проведення спінальної анестезії не зростає при збільшенні об’єму місцевого анестетика у пацієнтів високого зросту. 3. Підбір градаційної дози дозволяє більш прогнозовано і якісно застосовувати спінальну анестезію при ортопедо-травматологічних операціях.
Background. The development of a clear algorithm of a local anesthetic dosage for spinal anesthesia during surgeries on the lower extremities is an urgent issue, even after a century of using this method of analgesia. The aim of our study is to improve the efficiency and safety of spinal anesthesia during lower extremity surgery in orthopedic and trauma patients by developing a local anesthetic dosage algorithm. Materials and methods. The conducted study is based on the analysis of the bilateral spinal anesthesia methods in 75 patients with degree I–II ASA operational risk during orthopedic and trauma surgeries on the lower extremities who were divided into 3 study groups. Spinal anesthesia was performed using 0.5% bupivacaine, with the anesthetic dosage algorithm developed according to the patients’ height (group III) and the standard recommended dosage (group I, patients of short height, and group II, patients’ height > 180 cm). Results. When studying the hemodynamic indicators, the heart rate before surgery was as follows: in the first group, 73 ± 8 bpm, in the second group, 78 ± 6 bpm, in the third group, 79.32 ± 14.47 bpm. Thirty minutes after the injection of the anesthetic, the heart rate in the group 1 was 68 ± 5 bpm, and three hours after, it was 71 ± 9 bpm. In the group 2, the heart rate of patients 30 minutes after the injection of the anesthetic was 79 ± 7 bpm, three hours after, it was 84 ± 9 bpm. In the group 3, the heart rate of patients 30 minutes after the administration of the anesthetic was 71.56 ± 14.14 bpm, three hours after the injection, it was 71.280 ± 9.002 bpm. Data on systolic blood pressure before surgery was started were as follows: in the first group, 139.6 ± 12.3 mmHg, in the second group, 136.0 ± 9.6 mmHg, in the third group, 138.40 ± 16.18 mmHg. During the surgical intervention, blood pressure indicators in the group 1 were: 30 minutes after the introduction of the anesthetic — 113.0 ± 7.1 mmHg, 3 hours after — 122 ± 14 mmHg; in the second group: 30 minutes after the injection of the anesthetic — 138.0 ± 10.2 mmHg, 3 hours after — 141.0 ± 12.5 mmHg; in the third group: 30 minutes after the administration of the anesthetic — 102.48 ± 13.47 mmHg, 3 hours after the introduction — 118.2 ± 10.0 mmHg. The average duration of the sensory block in the group 1 was 182.5 ± 17.2 min, of the motor block — 130.0 ± 24.8 min; in patients of the group 2, the sensory block lasted 70.6 ± 13.1 min, and the motor block 23.3 ± 6.7 min; in the group 3, the duration of sensory block was 252.20 ± 74.32 min and of the motor block — 198.2 ± 59.0 min. Conclusions. 1. The use of small doses of hyperbaric bupivacaine does not affect hemodynamic parameters but reduces the quality and duration of anesthesia in tall patients. 2. The frequency of complications during spinal anesthesia does not increase with an increase in the volume of local anesthetic in tall patients. 3. Selection of graded dose allows for more predictable and qualitative application of spinal anesthesia during orthopedic and trauma surgeries.
спінальна анестезія; місцевий анестетик
spinal anesthesia; local anesthetic
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Хвисюк О.М., Фесенко В.С., Завеля М.І., Хвисюк О.М. Анестезія в ортопедії та травматології: навчальний посібник. Харків: Прапор, 2006. 416 с.
- Миллер Р. Анестезия Рональда Миллера. 7-е изд. В 2 томах. 2015. 3377 с.
- Галушко О.А., Шлапак І.П. Спосіб визначення дози місцевого анестетика при спинномозковій анестезії. Патент на корисну модель. Бюл. № 1, 2005.
- Глумчер Ф.С., Трещинский А.И. Руководство по анесте–зиологии: Учебное пособие. Київ: Медицина, 2008. 608 с.
- Sullivan J.T., Grouper S., Walker M.T., Parrish T.B., McCarthy R.J., Wong C.A. Lumbosacral cerebrospinal fluid volume in humans using three-dimensional magnetic resonance imaging. Anesth Analg. 2006 Nov. 103(5). 1306-10. DOI: 10.1213/01.ane.0000240886.55044.47.
- Jang Y.-E., Lee J.-H., Seo Y.-S., Yoon H.-C., Lee H.-S. et al. Lumbosacral and thoracolumbosacral cerebrospinal fluid volume changes in neonates, infants, children, and adolescents: A retrospective magnetic resonance imaging study. American Journal of Neuroradio–logy. 2017 May. 38 (5). 1061-1067. DOI: https://doi.org/10.3174/ajnr.A5134.
- Hogan Q.H., Prost R., Kulier A., Taylor M.L., Liu S., Mark L. Magnetic Resonance Imaging of Cerebrospinal Fluid Volume and the Influence of Body Habitus and Abdominal Pressure. Anesthesiology. 1996 June. 84. 1341-1349. DOI: https://doi.org/10.1097/00000542-199606000-00010.
- Enk D., Prien T., Van Aken H., Mertes N. Success rate of unilateral spinal anesthesia is dependent on injection flow. Reg. Anesth. Pain Med. 2001. 26. 5. 420-427.
- Serpell M.G., Gray W.M. Flow dynamics through spinal needles. Anaesthesia. 1997. 52. 3. P. 229-236.
- Casati A., Moizo E., Marchetti C., Vinciguerra F. Prospective, randomized, double-blind comparison of unilateral spinal anesthesia with hyperbaric bupivacaine, ropivacaine, or levobupivacaine for inguinal herniorrhaphy. Anesth. Analg. 2004. 99. 5. 1387-1392.
- Casati A., Fanelli G., Cappelleri G., Borghi B. Low dose hyperbaric bupivacaine for unilateral spinal anaesthesia. Can. J. Anaesth. 1998. 45. 9. 850-854.
- Kepekci A.B., Yavasca H.P., Daskaya H., İnal V. The Levels and Duration of Sensory and Motor Blockades of Spinal Anesthesia in Obese Patients That Underwent Urological Operations in the Lithotomy Position. BioMed Research International. 2015 (Article ID 453939). https://doi.org/10.1155/2015/453939.
- Lisowska B., Wiśniewski T., Olszewska M., Mał–dyk B., Ćwiek R., Słowińska I., Małdyk P. Znieczulenie podpajęczynó–wkowe — ocena porównawcza dwóch preparatów bupiwakainy, czy to samo to znaczy identyczne, czy tylko podobne? Anestezjologia i Ratownictwo. 2011. 5. 28-39.
- Milosavljevic S.B., Pavlovic A.P., Trpkovic S.V., Ilić A.N., Sekulic A.D. Influence of Spinal and General Anesthesia on the Metabo–lic, Hormonal, and Hemodynamic Response in Elective Surgical Patients. Med. Sci. Monit. 2014. 20. 1833-1840. doi: 10.12659/MSM.890981.
- Chinachoti T., Tritrakarn T. Prospective Study of Hypotension and Bradycardia during Spinal Anesthesia with Bupivacaine: Incidence and Risk Factors, Part Two. J. Med. Assoc. Thai. 2007. 90. 3. 492-501.