
Журнал «Боль. Суставы. Позвоночник» Том 13, №2, 2023
Вернуться к номеру
Вплив післяампутаційного больового синдрому на кровообіг у куксі кістки
Авторы: V.I. Shevchuk, Y.O. Bezsmertnyi, Y. Jiang, H.V. Bezsmertna, Y.S. Seheda, D.V. Bondarenko
Scientific and Research Institute of Rehabilitation of National Pirogov Memorial Medical University, Vinnytsia, Ukraine
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Справочник специалиста
Версия для печати
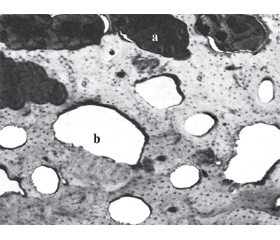
Актуальність. Відсоток незадовільних результатів ампутацій досі високий. При цьому особливе місце займає загоєння кісткового залишку — основного опорного елемента кукси. Мета: вивчити вплив післяампутаційного больового синдрому на характер кровообігу в куксі кістки. Матеріали та методи. На 54 кроликах проведено три серії дослідів з ампутацією стегна. У 1-й та 2-й серіях до кукси сідничного нерва підводили периневральний катетер. За його допомогою в 1-й серії протягом 20 діб щодня по 20 хвилин механічно подразнювали нерв, викликаючи больовий синдром. У 2-й серії через катетер в оточення нерва 20 днів щодня двічі на добу вводили 0,3 мл 1% лідокаїну. Тварини 3-ї серії слугували контролем. Строки спостереження становили 1, 3, 6 місяців. Метод дослідження — гістологічний, з інфузією туш-желатиновою сумішшю. Результати. У тварин 1-ї серії зафіксовано аваскулярність кінця кукси та кісткового мозку, бідність судинного русла та відсутність клітинного складу в гаверсових каналах, дистрофічні зміни жирового кісткового мозку, рарефікація, спонгізація, розсмоктування, надломи кісткової тканини. У дослідах 2-ї серії аваскулярність швидко минала, у період до трьох місяців наставала стабілізація ангіоархітектоніки. Реваскуляризація кукси кістки відбувалась за рахунок збережених джерел кровообігу (інтрамедулярна судинна мережа, окістя та прилеглі м’які тканини), анастомозуючих судин і позасудинних шляхів мікроциркуляції (підвищення судинної проникності, формування капілярів синусоїдного типу та тканинних кист). У більшості спостережень 3-ї серії процеси реваскуляризації були схожі з результатами 1-ї серії. Висновки. Післяампутаційний больовий синдром викликає різкі порушення макро- та мікроциркуляції. Його купірування протягом 20 днів після ампутації дозволяє значно нівелювати порушення кровообігу в куксі кістки.
Background. The percentage of unsatisfactory amputation results is still high. The healing of the bone remnant, the main supporting element of the residual limb, is of particular importance. The purpose was to study the effect of post-amputation pain syndrome on the nature of blood circulation in the bone residual limb. Materials and methods. Three series of experiments with amputation of the thigh were conducted on 54 rabbits. In the series 1 and 2, a perineural catheter was brought to the stump of the sciatic nerve. In series 1, for 20 days, every day for 20 minutes, mechanical irritation of the nerve was done, causing a pain syndrome using the perineural catheter. In series 2, 0.3 ml of 1% lidocaine was injected twice daily for 20 days; series 3 was a control. The follow-up periods were 1, 3, and 6 months. The study method was histological with the infusion of vessels with an ink-gelatin mixture. Results. Animals of the first series developed avascularity of the end of the stump and bone marrow, poor vascularity and absence of cellular composition in the Haversian canals, dystrophic changes in adipose bone marrow, rarefication, spongiosis, resorption, and bone fractures. In series 2, the avascularity passed quickly and by three months, the angioarchitectonics was stabilized. Revascularization of the bone stump occurs due to the preserved sources of blood circulation (intramedullary vascular network, periosteum and surrounding soft tissues) anastomosing vessels and extravascular pathways of microcirculation (increased vascular permeability, formation of sinusoidal capillaries and tissue cysts). In most observations of series 3, the processes of revascularization were similar to the results of the 1st series. Conclusions. Postamputation pain syndrome causes abrupt macro- and microcirculatory disturbances. Pain syndrome suppression allows to considerably level the arising circulatory disorders in the bone residual limb.
ампутація; больовий синдром; кукса кістки; кровообіг; регенерація
amputation; pain syndrome; bone stump; blood circulation; regeneration
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Ahmed A., Bhatnagar S., Mishra S. et al. Prevalence of phantom limb pain, stump pain, and phantom limb sensation among the amputated cancer patients in India: a prospective, observational study. Indian J. Palliat. Care. 2017. 23(1). 24-35. doi: 10.4103/0973-1075.197944.
- Ahuja V., Thapa D., Ghai B. Strategies for prevention of lower limb post-amputation pain: a clinical narrative review. J. Anaesthesiol. Clin. Pharmacol. 2018. 34(4). 439-449. doi: 10.4103/joacp.JOACP_126_17.
- Allami M., Faraji E., Mohammadzadeh F., Soroush M.R. Chronic musculoskeletal pain, phantom sensation, phantom and stump pain in veterans with unilateral below-knee amputation. Scand. J. Pain. 2019 Jul 4. doi: 10.1515/sjpain-2019-0045.
- Shevchuk V.I., Bezsmertnyi Y.O., Bezsmertna G.V., Dovgalyuk T.V., Jiang Y. Peculiar features of regeneration at the end of bone filing after amputation of a limb. World of Medicine and Biology. 2021. 1(75). 229-234. doi: 10.26724/2079-8334-2021-1-75-229-234.
- Shevchuk V.I., Bezsmertnyi Y.O., Bezsmertna H.V., Dovgalyuk T.V., Jiang Y. Reparative regeneration at the end of bone filing after ostoplastic amputation. Wiad. Lek. 2021. 74 (3 p. 1). 413-417. doi: 10.36740/WLek202103106.
- Bosanquet D.C., Glasbey J.C., Stimpson A., Williams I.M., Twina C.P. Systematic review and meta-analysis of the efficacy of perineural local anaesthetic catheters after major lower limb amputation. Eur. J. Vasc. Endovasc. Surg. 2015. 50(2). 241-249. doi: 10.1016/j.ejvs.2015.04.030.
- Buch N.S., Qerama E., Brix Finnerup N., Nikolajsen L. Neuromas and postamputation pain. Pain. 2020. 161(1). 147-155. doi: 10.1097/j.pain.0000000000001705.
- Buntragulpoontawee M., Pattamapaspong N., Tongprasert S. Multiple neuromas cause painful “Jum–ping Stump” in a transfemoral amputee: a case report. Int. J. Low Extrem. Wounds. 2016. 15(3). 271-273. doi: 10.1177/1534734616657964.
- Buchheit T., Hsia H.J., Cooter M. et al. The impact of surgical amputation and valproic acid on pain and functional trajectory: results from the veterans integrated pain evaluation research (VIPER) randomized, double-blinded placebo-controlled trial. Pain Med. 2019. 20(10). 2004-2017. doi: 10.1093/pm/pnz067.
- Dumanian G.A., Potter B.K., Mioton L.M. et al. Targeted muscle reinnervation treats neuroma and phantom pain in major limb amputees: a randomized clinical trial. Ann. Surg. 2019. 70(2). 238-246. doi: 10.1097/SLA.0000000000003088.
- Ayyaswamy B., Saeed B., Anand A., Chan L., Shetty V. Quality of life after amputation in patients with advanced complex regional pain syndrome: a syste–matic review. EFORT Open Rev. 2019. 4(9). 533-540. doi: 10.1302/2058-5241.4.190008.
- Harrison C., Epton S., Bojanic S., Green A.L., FitzGerald J.J. The efficacy and safety of dorsal root ganglion stimulation as a treatment for neuropathic pain: a lite–rature review. Neuromodulation: Technology at the Neural Interface. 2018. 21. 225-233. doi: org/10.1111/ner.12685.
- Culp C.J., Abdi S. Current understanding of phantom pain and its treatment. Pain Physician. 2022. 25. 941-957.
- Canavero S., Bonicalzi V. Central pain syndrome. Springer; 2018. 543. doi: 10.1007/978-3-319-56765-5.
- Lavrishcheva G.I., Onoprienko G.A. Morphological and clinical aspects of reparative regeneration of supporting organs and tissues. Medicine. 1996. 208 (in Ukrainian).
- Bezsmertny Yu.O. Morphological changes in tissue amputation of the lower end of the knuckle in case of muscular pain syndrome. Reports of Morphology. 2004. 2. 228231 (in Ukrainian).
- Knotkova H., Cruciani R.A., Tronnier V.M., –Rasche D. Current and future options for the management of phantom-limb pain. J. Pain Res. 2012. 5. 39-49. doi: 10.2147/JPR.S16733.
- Privitera R., Birch R., Sinisi M., Mihaylov I.R., Leech R., Anand P. Capsaicin 8% patch treatment for amputation stump and phantom limb pain: a clinical and functional MRI study. J. Pain Res. 2017. 10. 1623-1634. doi: 10.2147/JPR.S140925.
- Ramachandran V., Chunharas C., Marcus Z., Furnish T., Lin A. Relief from intractable phantom pain by combi–ning psilocybin and mirror visual-feedback (MVF). Neuroca–se. 2018. 24(2). 105-110. doi: 10.1080/13554794.2018.1468469.
- Hanyu-Deutmeyer A.A., Cascella M., Varacallo M. Phantom limb pain. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448188.
- Dommerholt J., Mayoral O., Thorp J.N. A critical overview of the current myofascial pain literature. Journal of Bodywork and Movement Therapies. 2021. 25. 261-271. doi: 10.1016/j.jbmt.2020.12.044.
- Fang J., Lian Y.H., Xie K.J., Cai S.N. Pharmacological interventions for phantom limb pain. Chin. Med. J. (Engl.). 2013. 126(3). 542-549.
- Brzeziński K., Rękas-Dudziak A.R., Maruszewska A. Pulsed radiofrequency as alternative method for phantom pain treatment. Case report. Clin. Case Rep. 2020. 8(10). 2060-2062. doi: 10.1002/ccr3.3110.
- Nardone R., Versace V., Sebastianelli L. et al. Trans–cranial magnetic stimulation in subjects with phantom pain and non-painful phantom sensations: a systematic review. Brain Research Bulletin. 2019. 148. 1-9. doi: 10.1016/j.brainresbull.2019.03.001.
- Bezsmertnyi Y., Shevchuk V., Jiang Y. The influence of post-amputation pain syndrome and intraosseous main vessels on the formation of limb bone stump. Orthopaedics, Traumatology and Prosthetics. 2023. 1–2. 20-25. doi: 10.15674/0030-598720221-220-25 (in Ukrainian).
- Karanikolas M., Aretha D., Tsolakis I. et al. Optimized perioperative analgesia reduces chronic phantom limb pain intensity, prevalence, and frequency: a prospective, randomized, clinical trial. Anesthesiology. 2011. 114(5). 1144-1154. doi: 10.1097/ALN.0b013e31820fc7d2.
- Goralsky L.P., Khomich V.T., Kononsky O.I. Fundamentals of histological techniques and morphofunctional methods for reaching the norm in pathology. Zhytomyr: Polissya, 2016. 288 (in Ukrainian).