
Журнал «Почки» Том 14, №1, 2025
Вернуться к номеру
Вагітність після трансплантації нирки: вплив на здоров’я матері та плода
Авторы: вагітність після трансплантації нирки; вагітність високого ризику
Рубрики: Нефрология
Разделы: Клинические исследования
Версия для печати
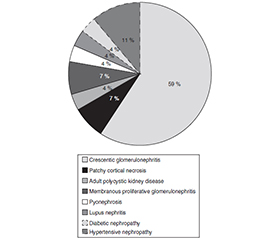
Актуальність. Вагітність у реципієнток трансплантованої нирки є високоризиковою через імуносупресію, наявні супутні захворювання і проблеми з функцією трансплантата. Оптимальні результати для матері й плода залежать від мультидисциплінарного підходу та сприятливих вихідних умов. Мета: визначити ідеальні умови вагітності в реципієнток трансплантованої нирки, оцінити вплив вагітності на здоров’я матері й функцію трансплантата. Матеріали та методи. Це було ретроспективне обсерваційне дослідження, проведене у відділенні акушерства та гінекології Інституту захворювань нирок та науково-дослідного центру (Ахмедабад, Індія) з 2014 року до листопада 2020 року. Проаналізовано 27 вагітностей у реципієнток трансплантованої нирки. Під час вагітності та після неї оцінювали нефрологічні параметри в матері, акушерські ускладнення й функцію трансплантата. Основні результати включали час між трансплантацією нирки та зачаттям, частоту народження живих дітей, ниркову функцію в матері та здоров’я новонародженого. Дані зібрані з клінічних записів і проаналізовані ретроспективно. Результати. Первинними кінцевими точками були інтервал між трансплантацією нирки та зачаттям, частота народження живих дітей і функція нирок матері до та після вагітності. Середній вік пацієнток на момент трансплантації становив 28,70 ± 3,82 року, середній вік на момент зачаття — 31,07 ± 2,57 року. Середній час між трансплантацією і зачаттям дорівнював 47 місяцям. Середній рівень креатиніну сироватки становив 1,13 ± 0,39 мг/дл під час зачаття й 1,09 ± 0,45 мг/дл після пологів. Шістнадцять вагітностей (59 %) завершилися народженням живих дітей. Поширеними ускладненнями були прееклампсія (6 випадків, 22,22 %), передчасні пологи (16 випадків, 59 %) та низька вага при народженні (9 випадків, 33,33 %). Кесарів розтин виконано 14 жінкам (52 %). Висновки. Вагітність у реципієнток трансплантованої нирки можлива при ретельному моніторингу і не має значного впливу на функцію трансплантата при дотриманні оптимальних умов. Результати залежать від адекватної функції нирок до вагітності, стабільної імуносупресивної терапії та мультидисциплінарного підходу.
Background. Pregnancy in kidney transplant recipients is high-risk due to immunosuppression, pre-existing comorbidities, and graft function concerns. Optimal maternal and foetal outcomes require a multidisciplinary approach and favourable baseline conditions. Objective: to identify ideal conditions for pregnancy in kidney transplant recipients and evaluate the impact of pregnancy on maternal and graft outcomes. Materials and methods. It was the retrospective observational study conducted at the Department of Obstetrics and Gynaecology of the Institute of Kidney Diseases and Research Centre (Ahmedabad, India) from 2014 to November 2020. A total of 27 pregnancies in kidney transplant recipients were analysed. Maternal nephrological parameters, obstetric complications, and graft function were assessed during and after pregnancy. Key outcomes measured included time between renal transplantation and conception, live birth rate, maternal renal function, and neonatal health. Data were collected from clinical records and analysed retrospectively. Results. The primary outcomes were the interval between renal transplantation and conception, live birth rate, and maternal renal function pre- and post-pregnancy. The mean age at transplantation was 28.70 ± 3.82 years, and the mean age at conception was 31.07 ± 2.57 years. The average time between transplantation and conception was 47 months. Median serum creatinine was 1.13 ± 0.39 mg/dL at conception and 1.09 ± 0.45 mg/dL postpartum. Sixteen pregnancies (59 %) resulted in live births. Common complications included preeclampsia (6 cases, 22.22 %), preterm delivery (16 cases, 59 %), and low birth weight (9 cases, 33.33 %). Caesarean section was performed in 14 patients (52 %). Conclusions. Pregnancy in kidney transplant recipients is feasible under strict monitoring and does not significantly affect graft function when optimal conditions are met. Outcomes are influenced by adequate pre-pregnancy renal function, stable immunosuppressive therapy, and multidisciplinary care.
post-kidney transplant pregnancy; high-risk pregnancy
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Sibanda N, Briggs JD, Davison JM, Johnson RJ, Rud–ge CJ. Pregnancy after organ transplantation: a report from the UK Transplant pregnancy registry. Transplantation. 2007 May 27;83(10):1301-7.
- Bramham K, Nelson-Piercy C, Gao H, Pierce M, Bush N, Spark P, et al. Pregnancy in renal transplant recipients: a UK national cohort study. Clin J Am Soc Nephrol. 2013 Feb;8(2):290-8.
- Mohammadi FA, Borg M, Gulyani A, McDonald SP, Jesudason S. Pregnancy outcomes and impact of pregnancy on graft function in women after kidney transplantation. Clin Transplant. 2017 Oct;31(10).
- Blencowe H, Lee AC, Cousens S, et al. Preterm birth-as–sociated neurodevelopmental impairment estimates at regional and global levels for 2010. Pediatr Res. 2013 Dec;74(Suppl 1):17-34.
- Schreiber-Zamora J, Szpotanska-Sikorska M, Drozdowska-Szymczak A, Czaplinska N, Pietrzak B, Wielgos M, et al. Neurological development of children born to mothers after kidney transplantation. J Matern Fetal Neonatal Med. 2017 Dec;3:1-5.
- Stanley CW, Gottlieb R, Zager R, Eisenberg J, Richmond R, Moritz MJ, et al. Developmental well-being in offspring of wo–men receiving cyclosporine post-renal transplant. Transplant Proc. 1999;31:241-2.
- Armenti VT, Moritz MJ, Cardonick EH, Davison JM. Immunosuppression in pregnancy: Choices for infant and maternal health. Drugs. 2002;62(16):2361-75.
- Deshpande NA, James NT, Kucirka LM, et al. Pregnancy outcomes in kidney transplant recipients: a systematic review and metaanalysis. Am J Transplant. 2011;11(11):2388-404.
- Umans JG. Medications during pregnancy: antihypertensives and immunosuppressives. Adv Chronic Kidney Dis. 2007;14:191-198.
- Baumwell S, Karumanchi SA. Pre-eclampsia: clinical manifestations and molecular mechanisms. Nephron Clin Pract. 2007;106:c72-c81.
- Del Mar Colon M, Hibbard JU. Obstetric considerations in the management of pregnancy in kidney transplant recipients. Adv Chronic Kidney Dis. 2007;14:168-177.
- McKay DB, Josephson MA. Pregnancy in recipients of solid organs: effects on mother and child. N Engl J Med. 2006;354:1281-1293.
- Oliveira LG, Sass N, Sato JL, Ozaki KS, Medina Pestana JO. Pregnancy after renal transplantation: a five-yr single-center experience. Clin Transplant. 2007;21:301-304.
- Gardella C, Brown ZA. Managing varicella zoster infection in pregnancy. Cleve Clin J Med. 2007;74:290-296.
- Davison JM, Lindheimer MD. Pregnancy and chronic kidney disease. Semin Nephrol. 2011 Jan;31(1):86-99.
- Teune MJ, Bakhuizen S, Gyamfi Bannerman C, et al. A systematic review of severe morbidity in infants born late preterm. Am J Obstet Gynecol. 2011;205(4): e371-4.
- Josephson MA, McKay DB. Considerations in the medical management of pregnancy in transplant recipients. Adv Chronic Kidney Dis. 2007;14:156-167.
- Chabria S. Aicardi’s syndrome: are corticosteroids teratogens? Arch Neurol. 1981;38:70.
- Lindheimer MD, Katz AI. Pregnancy in the renal transplant patients. Am J Kidney Dis. 1992;19:173-176.