
Журнал «Медицина неотложных состояний» Том 21, №3, 2025
Вернуться к номеру
Блокада площини випрямляча хребта при лапароскопічній холецистектомії: техніка виконання, систематичний огляд і метааналіз
Авторы: Чуклін С.М., Чуклін С.С.
Медичний центр Святої Параскеви, м. Львів, Україна
Рубрики: Медицина неотложных состояний
Разделы: Справочник специалиста
Версия для печати
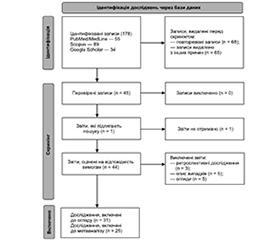
Актуальність. Хоча лапароскопічна холецистектомія (ЛХЕ) є малоінвазивною операцією, вона може викликати помірний або сильний післяопераційний біль. У рамках післяопераційної мультимодальної аналгезії регіонарна блокада все частіше застосовується у хірургії. Мета. Цей метааналіз мав на меті оцінити аналгетичну ефективність блокади площини випрямляча хребта у пацієнтів, які перенесли лапароскопічну холецистектомію. Матеріали та методи. Ми систематично проводили пошук у PubMed/MedLine, Scopus та Google Scholar до 2025 року. Усі рандомізовані клінічні випробування порівнювали ефективність блокади площини випрямляча хребта з іншими видами блокад для полегшення післяопераційного болю після ЛХЕ. Первинними (основними) результатами були: оцінка болю у спокої та при русі через 1–2, 6, 12 та 24 години після операції, доза фентанілу під час операції; вторинними — загальне вживання опіоїдів, час першого запиту на знеболювання та частота післяопераційної нудоти та блювання. Ми проаналізували всі дані за допомогою програмного забезпечення RevMan 5.4.1. Результати. Проведено огляд 31 рандомізованого контрольованого дослідження. У метааналіз включено 25 досліджень, в 16 з яких оцінювали ефективність блокади площини випрямляча хребта порівняно з групою пацієнтів без блокади, у 9 – з блокадою поперечної площини живота. Блокада площини випрямляча хребта суттєво зменшує інтенсивність болю в статичному і динамічному стані, потребу в інтраопераційному фентанілі, використання опіоїдів протягом 24 годин після операції та час до першого знеболювального порівняно з групою без блокади. Не було відмінностей між групами щодо нудоти та блювання. Блокада площини випрямляча хребта була ефективнішою у зниженні балів тяжкості болю у стані спокою, у всіх виміряних точках часу після операції, крім 12-ї год, ніж блокада поперечної площини живота, а під час руху — тільки на 6-й годині. Крім того, це призвело до меншого вживання еквівалента трамадолу протягом перших 24 год, збільшення часу до першого запиту на додаткове знеболювання порівняно з блокадою поперечної площини живота. Також не було суттєвих відмінностей у частоті післяопераційної нудоти та блювання. Висновки. Двобічна блокада площини випрямляча хребта під контролем ультразвуку може розглядатися як ефективний варіант післяопераційного знеболювання у дорослих, які перенесли лапароскопічну холецистектомію. Вона є дієвішою, ніж блокада поперечної площини живота.
Background. Although laparoscopic cholecystectomy is a minimally invasive procedure, it can cause moderate to severe postoperative pain. Regional block is increasingly used in surgery as part of postoperative multimodal analgesia. This meta-analysis aimed to evaluate the analgesic efficacy of erector spinae plane block (ESPB) in patients undergoing laparoscopic cholecystectomy. Materials and methods. We systematically searched PubMed/MEDLINE, Scopus, and Google Scholar up to 2025. All randomized controlled trials that compared the efficacy of ESPB with other types of blocks for relieving postoperative pain after laparoscopic cholecystectomy were included. The primary outcomes were pain scores at rest and on movement at 1–2, 6, 12, and 24 hours postoperatively, and intraoperative fentanyl dose. The secondary outcomes were total opioid consumption, first analgesia request time, and rates of postoperative nausea and vomiting. We analyzed all the data using RevMan 5.4.1 software. Results. A total of 31 randomized controlled trials were reviewed. Twenty-five studies were included in the meta-analysis, 16 of which compared ESPB with a no-block group, and 9 with the transversus abdominis plane (TAP) block. ESPB significantly reduced pain intensity in both static and dynamic states, intraoperative fentanyl requirements, 24-hour postoperative opioid consumption, and time to the first analgesia request compared with no-block group. There were no differences between groups in the incidence of nausea and vomiting. ESPB was more effective in reducing pain severity scores at rest in all measured postoperative time points except at 12 hours than TAP block, and on movement only at 6 hours. In addition, ESPB resulted in lower tramadol equivalent consumption within the first 24 hours and a longer time to the first request for additional analgesia compared with TAP block. There were no significant differences in the incidence of postoperative nausea and vomiting as well. Conclusions. Bilateral ultrasound-guided erector spinae plane block may be considered an effective option for postoperative analgesia in adults undergoing laparoscopic cholecystectomy. It is more effective than transverse abdominal plane block.
лапароскопічна холецистектомія; післяопераційний біль; блокада площини випрямляча хребта; блокада поперечної площини живота; огляд; метааналіз
laparoscopic cholecystectomy; postoperative pain; erector spinae plane block; transversus abdominis plane block; review; meta-analysis
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Gadiyaram S, Thota RK. Near-infrared fluorescence guided laparoscopic cholecystectomy in the spectrum of complicated gallstone disease. Medicine (Baltimore). 2022;101(42):e31170. doi: 10.1097/MD.0000000000031170.
- Nassar AH, Zanati HE, Ng HJ, Khan KS, Wood C. Open conversion in laparoscopic cholecystectomy and bile duct exploration: subspecialisation safely reduces the conversion rates. Surg Endosc. 2022;36:550-558. doi: 10.1007/s00464-021-08316-1.
- Wang W, Wang L, Gao Y. A meta-analysis of randomized controlled trials concerning the efficacy of transversus abdominis plane block for pain control after laparoscopic cholecystectomy. Front Surg. 2021;8:700318. doi: 10.3389/fsurg.2021.700318.
- Barazanchi AWH, MacFater WS, Rahiri JL, Tutone S, Hill AG, Joshi GP. Evidence-based management of pain after laparoscopic cholecystectomy: a PROSPECT review update. Br J Anaesth. 2018;121:787-803. doi: 10.1016/j.bja.2018.06.023.
- Karaca O, Pınar HU. Efficacy of ultrasound-guided erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: a retrospective cohort study. JARSS. 2020;28(3):179-187. doi: 10.5222/jarss.2020.02886.
- Jiang B, Ye S. Pharmacotherapeutic pain management in patients undergoing laparoscopic cholecystectomy: a review. Adv Clin Exp Med. 2022;31(11):1275-1288. doi: 10.17219/acem/151995.
- Sethi D, Garg G. Evaluation of postoperative analgesia of erector spinae plane block in elective laparoscopic cholecystectomy: a randomized controlled trial. Turk J Anaesthesiol Reanim. 2021;49(6):432-438. doi: 10.5152/TJAR.2021.878.
- Liu X, Hu J, Hu X, Li R, Li Y, Wong G, Zhang Y. Preemptive intravenous Nalbuphine for the treatment of post-operative visceral pain: a multicenter, double-blind, placebo-controlled, randomized clinical trial. Pain Ther. 2021;10(2):1155-1169. doi: 10.1007/s40122-021-00275-8.
- Karri SR, Jayaram K, Kumar A, Durga P. Comparison of the efficacy of gabapentin and memantine premedication in laparoscopic cholecystectomies for postoperative pain relief — A randomised placebo-controlled trial. Indian J Anaesth. 2021;65:539-544. doi: 10.4103/ija.IJA_140_21.
- Hannig KE, Jessen C, Soni UK, Borglum J, Bendtsen TF. Erector Spinae Plane Block for Elective Laparoscopic Cholecystectomy in the Ambulatory Surgical Setting. Case Rep Anesthesiol. 2018; Apr 1(2018):5492527. doi: 10.1155/2018/5492527.
- Chin KJ, Adhikary S, Sarwani N, Forero M. The analgesic efficacy of pre-operative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;72(4):452-460. doi: 10.1111/anae.13814.
- Ueshima H, Hiroshi O. Spread of local anesthetic solution in the erector spinae plane block. J Clin Anesth. 2018;45:23. doi: 10.1016/j.jclinane.2017.12.007.
- Wang Q, Huang L, Zeng W, Chen L, Zhao X. Assessment of Port-Specific Pain After Gynecological Laparoscopy: A Prospective Cohort Clinical Trial. J Laparoendosc Adv Surg Tech A. 2017;27(6):597-604. doi: 10.1089/lap.2016.0340.
- Zhao J, Peters L, Gelzinnis S, Carroll R, Nolan J, Di Sano S, Pockney P, Smith S. Post-discharge opioid prescribing after laparoscopic appendicectomy and cholecystectomy. ANZ J Surg. 2020;90:1014-1018. https://doi.org/10.1111/ans.15882.
- Mak MHW, Chew WL, Junnarkar SP, Woon WWL, Low JK, Huey TCW, Shelat VG. Patient reported outcomes in elective laparoscopic cholecystectomy. Ann Hepatobiliary Pancreat Surg. 2019;23(1):20-33. doi: 10.14701/ahbps.2019.23.1.20.
- Lockett MA, Ward RC, McCauley JL, Taber DJ, Gebregziabher M, Cina RA, Basco WT Jr, Mauldin PD, Ball SJ. New chronic opioid use in Medicaid patients following cholecystectomy. Surg Open Sci. 2022;9:101-108. doi: 10.1016/j.sopen.2022.05.009.
- Eftekhariyazdi M, Ansari M, Darvishi-Khezri H, Zardosht R. Pharmacological Methods of Postoperative Pain Management After Laparoscopic Cholecystectomy: A Review of Meta-analyses. Surg Laparosc Endosc Percutan Tech. 2020;30(6):534-541. doi: 10.1097/SLE.0000000000000824.
- Macintyre PE, Quinlan J, Levy N, Lobo DN. Current Issues in the Use of Opioids for the Management of Postoperative Pain: A Review. JAMA Surg. 2022;157(2):158-166. doi: 10.1001/jamasurg.2021.6210.
- Mounika V, Sahu L, Mishra K, Mohapatra PS. A Comparative Evaluation of Post-operative Pain Management Using Erector Spinae Plane Block and Oblique Transverse Abdominis Plane Block in Patients Undergoing Laparoscopic Cholecystectomy. Cureus. 2023;15(3):e35750. doi: 10.7759/cureus.35750.
- Altıparmak B, Korkmaz Toker M, Uysal AI, Kuşçu Y, Gümüş Demirbilek S. Ultrasound-guided erector spinae plane block versus oblique subcostal transversus abdominis plane block for postoperative analgesia of adult patients undergoing laparoscopic cholecystectomy: randomized, controlled trial. J Clin Anesth. 2019;57:31-36. doi: 10.1016/j.jclinane.2019.03.012.
- Aygun H, Kavrut Ozturk N, Pamukcu AS, Inal A, Kiziloglu I, Thomas DT, Tulgar S, Nart A. Comparison of ultrasound guided Erector Spinae Plane Block and quadratus lumborum block for postoperative analgesia in laparoscopic cholecystectomy patients; a prospective randomized study. J Clin Anesth. 2020;62:109696. doi: 10.1016/j.jclinane.2019.109696.
- Cesur S, Hadi Ufuk YRKL, Aksu C, Ku A. Bilateral versus unilateral erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: a randomized controlled study. Braz J Anesthesiol. 2023;73(1):72-77. doi: 10.1016/j.bjane.2021.04.020.
- Vrsajkov V, Ilić N, Uvelin A, Ilić R, Lukić-Šarkanović M, Plećaš-Đurić A. Erector spinae plane block reduces pain after laparoscopic cholecystectomy. Anaesthesist. 2021;70(Suppl 1):48-52. doi: 10.1007/s00101-021-01015-5.
- Ozdemir H, Araz C, Karaca O, Turk E. Comparison of Ultrasound-Guided Erector Spinae Plane Block and Subcostal Transversus Abdominis Plane Block for Postoperative Analgesia after Laparoscopic Cholecystectomy: A Randomized, Controlled Trial. J Invest Surg. 2022;35(4):870-877. doi: 10.1080/08941939.2021.1931574.
- Liu H, Brown M, Sun L, Patel SP, Li J, Cornett EM, Urman RD, Fox CJ, Kaye AD. Complications and liability related to regional and neuraxial anesthesia. Best Pract Res Clin Anaesthesiol. 2019;33(4):487-497. doi: 10.1016/j.bpa.2019.07.007.
- Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621-627. doi: 10.1097/AAP.0000000000000451.
- Cui Y, Wang Y, Yang J, Ran L, Zhang Q, Huang Q, Gong T, Cao R, Yang X. The Effect of Single-Shot Erector Spinae Plane Block (ESPB) on Opioid Consumption for Various Surgeries: A Meta-Analysis of Randomized Controlled Trials. J Pain Res. 2022;15:683-699. doi: 10.2147/JPR.S346809.
- Chin KJ, El-Boghdadly K. Mechanisms of action of the erector spinae plane (ESP) block: a narrative review. Can J Anaesth. 2021;68(3):387-408. doi: 10.1007/s12630-020-01875-2.
- De Cassai A, Bonvicini D, Correale C, Sandei L, Tulgar S, Tonetti T. Erector spinae plane block: a systematic qualitative review. Minerva Anestesiol. 2019;85(3):308-319. doi: 10.23736/S0375-9393.18.13341-4.
- Urits I, Charipova K, Gress K, Laughlin P, Orhurhu V, Kaye AD, Viswanath O. Expanding Role of the Erector Spinae Plane Block for Postoperative and Chronic Pain Management. Curr Pain Headache Rep. 2019;23(10):71. doi: 10.1007/s11916-019-0812-y.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178-189. doi: 10.1016/j.jclinepi.2021.03.001.
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane, 2024. Available from: www.training.cochrane.org/handbook.
- Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi: 10.1186/1471-2288-14-135.
- Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta-analyses can provide accurate results. J Clin Epidemiol. 2006;59(1):7-10. doi: 10.1016/j.jclinepi.2005.06.006.
- El-Boghdadly K, Wolmarans M, Stengel AD, Albrecht E, Chin KJ, Elsharkawy H, et al. Standardizing nomenclature in regional anesthesia: an ASRA-ESRA Delphi consensus study of abdominal wall, paraspinal, and chest wall blocks. Reg Anesth Pain Med. 2021;46(7):571-580. doi: 10.1136/rapm-2020-102451.
- Kot P, Rodriguez P, Granell M, Cano B, Rovira L, Morales J, Broseta A, Andrés J. The erector spinae plane block: a narrative review. Korean J Anesthesiol. 2019;72(3):209-220. doi: 10.4097/kja.d.19.00012.
- De Cassai A, Tonetti T. Local anesthetic spread during erector spinae plane block. J Clin Anesth. 2018;48:60-61. doi: 10.1016/j.jclinane.2018.05.003.
- Adhikary SD, Bernard S, Lopez H, Chin KJ. Erector spinae plane block versus retrolaminar block: a magnetic resonance imaging and anatomical study. Reg Anesth Pain Med. 2018;43:756-762. doi: 10.1097/AAP.0000000000000798.
- Vidal E, Giménez H, Forero M, Fajardo M. Erector spinae plane block: a cadaver study to determine its mechanism of action. Rev Esp Anestesiol Reanim. 2018;65:514-519. doi: 10.1016/j.redar.2018.07.004.
- Sørenstua M, Zantalis N, Raeder J, Vamnes JS, Leo–nardsen AL. Spread of local anesthetics after erector spinae plane block: an MRI study in healthy volunteers. Reg Anesth Pain Med. 2023;48(2):74-79. doi: 10.1136/rapm-2022-104012.
- Hassanein A, Abdel-Haleem M, Mohamed SR. Regional –Analgesia for Laparoscopic Cholecystectomy Using Ultrasound-guided Quadratus Lumborum Block or Erector Spinae Block: A Randomized Controlled Trial. Pain Physician. 2023;26(3):E133-E141. PMID: 37192231.
- Rahimzadeh P, Faiz SHR, Salehi S, Imani F, Mueller AL, Sabouri AS. Unilateral Right-Sided Ultrasound-Guided Erector Spinae Plane Block for Post-Laparoscopic Cholecystectomy Analgesia: A Randomized Control Trial. Anesth Pain Med. 2022;12(6):e132152. doi: 10.5812/aapm-132152.
- Peker K, Akçaboy ZN, Aydın G, Gençay I, Şahin AT, Koçak YF, Peker SA. The Effect of Erector Spinae Plane Block on Laparoscopic Cholecystectomy Anesthesia: Analysis of Opioid Consumption, Sevoflurane Consumption, and Cost. J Laparoendosc Adv Surg Tech A. 2020;30(7):725-729. doi: 10.1089/lap.2019.0809.
- Lu H, Xie Q, Ye W, Zhou Z, Lei Z. Ultrasound-guided erector spinae plane block for postoperative analgesia in Chinese patients undergoing laparoscopic cholecystectomy: a double-blind randomized controlled trial. Langenbecks Arch Surg. 2023;408(1):111. doi: 10.1007/s00423-023-02834-3.
- Yılmaz ET, Gülmez DD, Apan A, Keles BO, Coşkun M, Döger C, et al. A novel comparison of erector spinae plane block and paravertebral block in laparoscopic cholecystectomy. Rev Assoc Med Bras (1992). 2024;70(3):e20231457. doi: 10.1590/1806-9282.20231457.
- Yildiz M, Kozanhan B, Iyisoy MS, Canıtez A, Aksoy N, Eryigit A. The effect of erector spinae plane block on postoperative analgesia and respiratory function in patients undergoing laparoscopic cholecystectomy: A double-blind randomized controlled trial. J Clin Anesth. 2021;74:110403. doi: 10.1016/j.jclinane.2021.110403.
- Joshi Y, Ramakrishnan P, Jindal P, Sachan PK. Ultrasound-guided erector spinae plane block versus port site infiltration for postoperative pain and quality of recovery in adult patients undergoing laparoscopic cholecystectomy: An assessor-blinded randomised controlled trial. Indian J Anaesth. 2023;67(8):714-719. doi: 10.4103/ija.ija_556_22.
- Verma R, Srivastava D, Saxena R, Singh TK, Gupta D, Agarwal A, Mishra P. Ultrasound-guided Bilateral Erector Spinae Plane Block for Postoperative Analgesia in Laparoscopic Cholecystectomy: A Randomized Controlled Trial. Anesth Essays Res. 2020;14(2):226-232. doi: 10.4103/aer.AER_41_20.
- Sethi D, Garg G. Erector spinae block for laparoscopic cholecystectomy Turk J Anaesthesiol Reanim. 2021;49(6):432-438. doi: 10.5152/TJAR.2021.878.
- Ibrahim M. Erector Spinae Plane Block in Laparoscopic Cholecystectomy, Is There a Difference? A Randomized Controlled Trial. Anesth Essays Res. 2020;14(1):119-126. doi: 10.4103/aer.AER_144_19.
- Canıtez A, Kozanhan B, Aksoy N, Yildiz M, Tutar MS. Effect of erector spinae plane block on the postoperative quality of recovery after laparoscopic cholecystectomy: a prospective double-blind study. Br J Anaesth. 2021;127(4):629-635. doi: 10.1016/j.bja.2021.06.030.
- Lin Z, Chen C, Xie S, Chen L, Yao Y, Qian B. Systemic lidocaine versus erector spinae plane block for improving quality of recovery after laparoscopic cholecystectomy: A randomized controlled trial. J Clin Anesth. 2024;97:111528. doi: 10.1016/j.jclinane.2024.111528.
- Tulgar S, Kapakli MS, Senturk O, Selvi O, Serifsoy TE, Ozer Z. Evaluation of ultrasound-guided erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: A prospective, randomized, controlled clinical trial. J Clin Anesth. 2018;49:101-106. doi: 10.1016/j.jclinane.2018.06.019.
- Mahdy MM, Abdelhakeem EE, Fawzy AM, Abbas MS. Comparison of analgesic efficacy of ultrasound-guided erector spinae block with port site infiltration following laparoscopic cholecystectomy. Egyptian Journal of Anaesthesia. 2023;39(1):528-537. doi: 10.1080/11101849.2023.2230049.
- Gupta A, Angral R, Kalsotra SK, Chander AM, Sharma RR. A comparative evaluation of ultrasound guided dual transversus abdominis plane block versus erector spinae plane block for postoperative analgesia in patients undergoing laparoscopic cholecystectomy: A randomised prospective study. Indian J Clin Anaesth. 2024;11(3):309-315. doi: 10.18231/j.ijca.2024.060.
- Aksu C, Kuş A, Yörükoğlu HU, Kılıç CT, Gürkan Y. The Effect of Erector Spinae Plane Block on Postoperative Pain Following Laparoscopic Cholecystectomy: A Randomized Controlled Study. JARSS. 2019;27(1):9-14. doi: 10.5222/jarss.2019.14632.
- Kwon HM, Kim DH, Jeong SM, Choi KT, Park S, Kwon HJ, Lee JH. Does Erector Spinae Plane Block Have a Visceral Analgesic Effect? A Randomized Controlled Trial. Sci Rep. 2020;10(1):8389. doi: 10.1038/s41598-020-65172-0.
- Engineer SR, Devanand A, Kulkarni M. Comparative study of the efficacy of ultrasound-guided erector spinae block and oblique subcostal transversus abdominis plane block for postoperative analgesia after laparoscopic cholecystectomy. Ain-Shams Journal of Anesthesiology. 2022;14:84. doi: 10.1186/s42077-022-00285-4.
- Altiparmak B, Toker MK, Uysal Aİ, Kuşçu Y, Demirbilek SG. Efficacy of ultrasound-guided erector spinae plane block for analgesia after laparoscopic cholecystectomy: a randomized controlled trial. Braz J Anesthesiol. 2019;69(6):561-568. doi: 10.1016/j.bjan.2019.09.001.
- Gangadharaiah R, Rani DD, Venkatesh N, Nithish S, Nethra SS. Efficacy of Ultrasound Guided Bilateral Erector Spinae Block for Postoperative Analgesia in Patients Undergoing Laparoscopic Cholecystectomy under General Anaesthesia: A Randomised Control Study. Karnataka Anaesthesia Journal. 2019;17(1&2):13-21. doi: 10.4103/kaj/2019/v17i1-2/158805.
- Routray SS, Mohanty R, Pradhan K, Pani S. Evaluation of efficacy of ultrasound guided erector spinae plane block and oblique subcostal transversus abdominis plane block for postoperative analgesia in laparoscopic cholecystectomy. Panacea J Med Sci. 2020;10(2):128-134. doi: 10.18231/j.pjms.2020.028.
- Sahu L, Behera SK, Satapathy GC, Saxena S, Priyadarshini S, Sahoo RK. Comparison of Analgesic Efficacy of Erector Spinae and Oblique Subcostal Transverse Abdominis Plane Block in Laparoscopic Cholecystectomy. Journal of Clinical and Diagnostic Research. 2021;15(9):UC09-UC13. doi: 10.7860/JCDR/2021/50795.15380.
- Sifaki F, Mantzoros I, Koraki E, Bagntasarian S, Christidis P, Theodoraki K. The Effect of Ultrasound-guided Bilateral Erector Spinae Plane Block With and Without Dexmedetomidine on Intra-operative and Postoperative Pain in Laparoscopic Cholecystectomies: A Randomized, Controlled, Double-blind, Prospective Trial. Pain Physician. 2022 Oct;25(7):E999-E1008. PMID: 36288585.
- Ali M, Yasin B, Khan S, Ali I, Abdullah H, Tarar HM. Ultrasound-Guided Erector Spinae Plane Block versus Oblique Subcostal Transversus Abdominis Plane Block for Post-Operative Analgesia of Adult Patients Undergoing Laparoscopic Cholecystectomy. Pak Armed Forces Med J. 2023;73(5):1245-1248. doi: 10.51253/pafmj.v73i5.6983.
- Bezen BA, Sıvacı R, Akıcı M, Bakı ED. Comparison of Ultrasound-Guided Thoracic Paravertebral Block and Erector Spinae Plane Block for Postoperative Analgesia After Laparoscopic Cholecystectomy. Cyprus J Med Sci. 2024;9(3):161-166. doi: 10.4274/cjms.2024.2023-65.
- Boezaart AP, Smith CR, Chembrovich S, Zasimovich Y, Ser-ver A, Morgan G, et al. Visceral versus somatic pain: an educational review of anatomy and clinical implications. Reg Anesth Pain Med. 2021;46(7):629-636. doi: 10.1136/rapm-2020-102084.
- Lee H, Askar A, Makanji D, Ranjha K, Karki BB, Courcol J, Kukreja Y, Niraj G. The incidence of post cholecystectomy pain (PCP) syndrome at 12 months following laparoscopic cholecystectomy: a prospective evaluation in 200 patients. Scand J Pain. 2023;24(1). doi: 10.1515/sjpain-2023-0067.
- Liheng L, Siyuan C, Zhen C, Changxue W. Erector Spinae Plane Block versus Transversus Abdominis Plane Block for Postoperative Analgesia in Abdominal Surgery: A Systematic Review and Meta-Analysis. J Invest Surg. 2022;35(9):1711-1722. doi: 10.1080/08941939.2022.2098426.
- Akter B, Bahar AA, Ahmed J, Islam MT, Zana K, Alam MR, Rahman M, Mowla G, Hassan AN, Kabir A. Port-site infiltration of bupivacaine in reduction of postoperative pain after laparoscopic cholecystectomy. Int J Surg Sci. 2021;5(2):135-138. doi: 10.33545/surgery.2021.v5.i2c.674.
- Elsharkawy H, Pawa A, Mariano ER. Interfascial Plane Blocks: Back to Basics. Reg Anesth Pain Med. 2018;43(4):341-346. doi: 10.1097/AAP.0000000000000750.
- Elsharkawy H, Bajracharya GR, El-Boghdadly K, Drake RL, Mariano ER. Comparing two posterior quadratus lumborum block approaches with low thoracic erector spinae plane block: an anatomic study. Reg Anesth Pain Med. 2019 Mar 28:rapm-2018-100147. doi: 10.1136/rapm-2018-100147.
- Slinchenkova K, Lee K, Choudhury S, Sundarapandiyan D, Gritsenko K. A Review of the Paravertebral Block: Benefits and Complications. Curr Pain Headache Rep. 2023;27(8):203-208. doi: 10.1007/s11916-023-01118-1.