
Журнал «Боль. Суставы. Позвоночник» Том 15, №2, 2025
Вернуться к номеру
Особливості перебігу псоріатичного артриту у пацієнтів з гіперурикемією або подагрою
Авторы: Борткевич О.П. (1), Сидоренко Д.М. (1), Мітченко О.І. (1), Воронков Л.Г. (1), Крилова А.С. (2)
(1) - ДУ «ННЦ «Інститут кардіології, клінічної та регенеративної медицини імені академіка М.Д. Стражеска Національної академії медичних наук України», м. Київ, Україна
(2) - Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
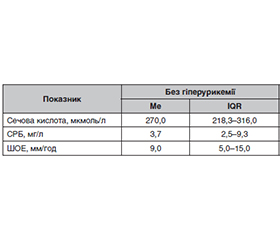
Актуальність. Протягом останніх років дослідження вказують на можливий зв’язок між підвищеним рівнем сечової кислоти та тяжчим перебігом псоріатичного артриту (ПсА), зокрема більш частим розвитком ерозивних змін. Мета: визначити клініко-лабораторні та рентгенологічні особливості перебігу ПсА у пацієнтів із гіперурикемією або подагрою. Матеріали та методи. Проведено ретроспективний аналіз історій хвороби 98 пацієнтів, хворих на ПсА, зі стаціонару ДУ «ННЦ ім. акад. М.Д. Стражеска НАМН України» у 2023–2025 рр. Пацієнти з ПсА були поділені та групи залежно від наявності нормо- чи гіперурикемії, подагри та виду базисної терапії. Аналізували загальноклінічні, лабораторні (визначення маркерів запалення, рівня урикемії), інструментальні (рентгенологічне дослідження) показники. Застосовували методи анкетування та біомедичної статистики. Результати. Порівняно з пацієнтами з нормоурикемією гіперурикемічна група частіше мала чоловічу стать (73 проти 89 %). Кількість ентезитів (анамнестично) була вищою у гіперурикемічній групі, ніж у групі нормоурикемії (41 проти 23 %, p = 0,04). У першій групі ШОЕ не перевищувала норму та становила 9,00 (IQR 5,00–15,00) мм/год, у другій групі вона була вищою (12,00 (IQR 5,00–21,50) мм/год), хоч і статистично невірогідною. Рівень С-реактивного білка (СРБ) статистично вищим був у групі гіперурикемії. У пацієнтів з подагрою виявлено вищі значення сечової кислоти (медіана — 549,0 ммоль/л), ШОЕ (медіана — 16,00 мм/год) та СРБ (медіана — 11,35 мг/л). У групі гіперурикемії частіше діагностували вищу ренгенологічну стадію ПсА. Рівні сечової кислоти в об’єднаній групі біологічної та комбінованої терапії (281,0 (IQR 223,0–336,0) мкмоль/л) були вірогідно нижчими (р = 0,049) порівняно з показниками осіб, які отримували синтетичну терапію. Висновки. Пацієнти з ПсА мали часту коморбідність з гіперурикемією та подагрою (30 %), що впливало на тяжчий перебіг хвороби, більше ентезитів, вищу рентгенологічну стадію та рівні показників запалення, що слід враховувати в менеджменті хворих.
Background. Recent studies indicate a possible link between elevated uric acid levels and a more severe course of psoriatic arthritis (PsA), in particular, more frequent development of erosive changes. The purpose was to determine the clinical, laboratory, and radiological features of PsA in patients with hyperuricemia or gout. Materials and methods. A retrospective analysis of the medical records of 98 patients with PsA, which were divided into groups based on normo/hyperuricemia/presence of gout and type of suppurative therapy. The following parameters were analyzed: general clinical, laboratory (determination of inflammatory markers, urea level), and instrumental (X-ray examination) parameters. Methods of questionnaire and biomedical statistics were used. Results. Compared with patients with normouricemia, the hyperuricemic group was more often male (73 vs. 89 %). The number of enthesitis (anamnestic) was higher in the hyperuricemic group than in the normouricemic group (41 vs. 23 %, p = 0.04). In the first group, the erythrocyte sedimentation rate (ESR) did not exceed the normal range and was 9.00 (IQR 5.0–15.0) mm/h, in the second group it was higher (12.00 (IQR 5.0–21.5) mm/h), although statistically insignificant. The level of C-reactive protein (CRP) was statistically higher in the hyperuricemia group. Patients with gout had higher values of uric acid (median — 549.0 mmol/l), ESR (median – 16.0 mm/h) and CRP (median — 11.35 mg/l). In the hyperuricemia group, the highest radiological stage was diagnosed more often. The significant lower level of uric acid (281.0 (IQR 223.0–336.0) mmol/l) was observed in the combined group of biological and combined therapy (p = 0.049) compared with synthetic therapy. Conclusion. Patients with PsA had a frequent comorbidity with hyperuricemia and gout (30 %), which influenced the more severe course of the disease, more enthesitis, higher radiological stage and inflammation levels, which should be considered in patient management.
серонегативні спондилоартрити; псоріатичний артрит; подагра; гіперурикемія; базисна терапія
seronegative spondyloarthritis; psoriatic arthritis; gout; hyperuricemia; basic therapy
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Ogdie A, Weiss P. The Epidemiology of Psoriatic Arthritis. Rheum Dis Clin North Am. 2015;41(4):545-568. doi: 10.1016/j.rdc.2015.07.001.
- Mease PJ, Gladman DD, Papp KA, Khraishi MM, Thaçi D, Behrens F, et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J Am Acad Dermatol. 2013;69(5):729-735. doi: 10.1016/j.jaad.2013.07.023.
- Gladman DD, Antoni C, Mease P, Clegg DO, Nash P. Psoriatic arthritis: Epidemiology, clinical features, course, and outcome. Ann Rheum Dis. 2005;64(Suppl 2):ii14-ii17. doi: 10.1136/ard.2004.032482.
- Widawski L, Fabacher T, Spielmann L, Gottenberg JE, Sibilia J, Duret PM, Messer L. Psoriatic arthritis with hyperuricemia: more peripheral, destructive, and challenging to treat. Clin Rheumatol. 2022;41(5):1421-1429. doi: 10.1007/s10067-022-06061-x.
- Felten R, Widawski L, Duret PM, Spielmann L, Mes–ser L. Convergence of Psoriatic Arthritis and Hyperuricemia: A Review of Emerging Data from This New Concept Called “Psout”. Gout Urate Crystal Depos Dis. 2025;3(1):4. doi: 10.3390/gucdd3010004.
- Perković D, Petrić M, Maleš M, Erceg Maleš I, Radić M. Biological Disease-Modifying Antirheumatic Drugs Decrease Uric Acid Levels in the Sera of Patients with Psoriatic Arthritis. Curr Issues Mol Biol. 2025;47(3):142. doi: 10.3390/cimb47030142.
- Felten R, Duret PM, Gottenberg JE, Spielmann L, Messer L. At the crossroads of gout and psoriatic arthritis: “psout”. Clin Rheumatol. 2020;39(5):1405-1413. doi: 10.1007/s10067-020-04981-0.
- Sherri A, Mortada MM, Makowska J, Sokolowska M, Lewandowska-Polak A. Understanding the interplay between psoriatic arthritis and gout: “Psout”. Rheumatol Int. 2024;44(12):2699-2709. doi: 10.1007/s00296-024-05729-8.
- Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet. 2016;388(10055):2039-2052. doi: 10.1016/S0140-6736(16)00346-9.
- Fisher MC, Rai SK, Lu N, Zhang Y, Choi HK. The unclosing premature mortality gap in gout: A general population-based study. Ann Rheum Dis. 2017;76(7):1289-1294. doi: 10.1136/annrheumdis-2016-210547.
- Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P, Mielants H; CASPAR Study Group. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Rheum. 2006;54(8):2665-2673. doi: 10.1002/art.21972.
- Chu BBR, Pereira da Cunha JPVV, Marcon JMT, de Arruda Prado LE, Rosa FLS, Leitão JM, et al. Does Disease Activity Influence the Levels of Uric Acid in Psoriatic Arthritis? Open Rheumatol J. 2021;15:57-64. doi: 10.2174/1874312902115010057.
- Lai TL, Yim CW, Wong PY, Leung MC, Ng WL. Hyperuricemia in Asian psoriatic arthritis patients. Int J Rheum Dis. 2018;21(4):843-849. doi: 10.1111/1756-185X.13265.
- Gudu T, Peltea A, Balanescu A, Bojinca V, Opris D, Predeteanu D, Ionescu R. AB0790 Hyperuricemia in psoriatic arthritis: Prevalence and associated factors. Ann Rheum Dis. 2017;76(Suppl 2):1333-1334. doi: 10.1136/annrheumdis-2017-eular.5744.
- Al Johani R, Polachek A, Ye JY, Chandran V, Gladman DD. Characteristic and Outcome of Psoriatic Arthritis Patients with Hyperuricemia. J Rheumatol. 2018;45(2):213-217. doi: 10.3899/jrheum.170906.
- Moshrif A, Mosallam A, Mohamed EE, Gouda W, Doma M. Subclinical enthesopathy in patients with psoriasis and its association with other disease parameters: a power Doppler ultrasonographic study. Eur J Rheumatol. 2017;4(1):24-28. doi: 10.5152/eurjrheum.2017.16063.
- Pineda C, Amezcua-Guerra LM, Solano C, Rodriguez-Henríquez P, Hernández-Díaz C, Vargas A, et al. Joint and tendon subclinical involvement suggestive of gouty arthritis in asymptomatic hyperuricemia: an ultrasound controlled study. Arthritis Res Ther. 2011;13(1):R4. doi: 10.1186/ar3223.
- Hagino T, Saeki H, Fujimoto E, Kanda N. Effects of Biologic Therapy on Laboratory Indicators of Cardiometabolic Diseases in Patients with Psoriasis. J Clin Med. 2023;12(6):1934. doi: 10.3390/jcm12061934.
- Zheng Zhao, Lin Cai, Si Zhang, Heng Zhang, Xiaoyang Liu, Chenglong Li, Yan Zhao, Jianzhong Zhang. Effects of secukinumab and adalimumab on serum uric acid level in patients with plaque psoriasis. Chin Med J (Engl). 2022 Jul 15;135(12):1438-1443. doi: 10.1097/CM9.0000000000002130.
- Virdis A, Masi S, Casiglia E, Tikhonoff V, Cicero AFG, Ungar A, et al. Identification of the Uric Acid Thresholds Predicting an Increased Total and Cardiovascular Mortality Over 20 Years. Hypertension. 2020; 75(2):302-308. doi: 10.1161/HYPERTENSIONAHA.119.13875.