
Журнал «Медицина неотложных состояний» Том 21, №7, 2025
Вернуться к номеру
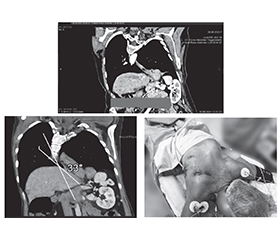
Клінічний випадок: мініінвазивна езофагектомія за McKeown у пацієнтки зі сколіозом ІІІ ступеня
Авторы: Усенко О.Ю., Сидюк А.В., Сидюк О.Є., Клімас А.С., Чечіль С.І., Дикань А.А.
ДУ «Національний науковий центр хірургії та трансплантології імені О.О. Шалімова НАМН України»,
м. Київ, Україна
Рубрики: Медицина неотложных состояний
Разделы: Справочник специалиста
Версия для печати
Рак стравоходу — онкологічне захворювання, яке характеризується високою летальністю та часто пізньою діагностикою. Основними гістологічними формами є плоскоклітинний рак та аденокарцинома. Клінічно хворі можуть скаржитися на прогресуючу дисфагію, втрату маси тіла, біль за грудниною або в спині, охриплість голосу. Діагностика включає ендоскопію з біопсією, КТ, ПЕТ-КТ для оцінки стадії пухлини. Лікування залежить від стадії: комбінована терапія (хіміотерапія, променева терапія + хірургія) є стандартом при локалізованому раку. Хірургічне втручання — езофагектомія — залишається основним методом лікування, особливо у пацієнтів без віддалених метастазів. Мініінвазивна езофагектомія за McKeown — це комбінований хірургічний підхід до видалення стравоходу при злоякісному новоутворенні, що поєднує лапароскопічний етап із торакоскопічним доступом, а також цервікальний етап. Переваги включають зменшення післяопераційного болю, менш тривале перебування в стаціонарі, швидше відновлення та зниження частоти ускладнень. Але наявність тяжких супутніх патологій, як-от сколіоз III ступеня, значно ускладнює оперативне втручання та потребує ретельного анестезіологічного та хірургічного планування. За умов мультидисциплінарного підходу — з урахуванням анестезіологічного забезпечення, адаптації етапів операції до анатомічних змін та продуманого післяопераційного ведення — можливо досягти позитивного результату навіть у складних клінічних ситуаціях.
Esophageal cancer is an oncological disease characterized by high mortality and often late diagnosis. The main histological forms are squamous cell carcinoma and adenocarcinoma. Clinically, patients may complain of progressive dysphagia, weight loss, pain behind the sternum or in the back, and hoarseness. Diagnosis includes endoscopy with biopsy, computed tomography, and positron emission tomography-computed tomography to assess the stage of the tumor. Treatment depends on the stage: combination therapy (chemotherapy, radiation therapy + surgery) is the standard for localized cancer. Surgical intervention — esophagectomy — remains the main treatment, especially in patients without distant metastases. Minimally invasive McKeown esophagectomy is a combined surgical approach to removing the esophagus in malignant neoplasms, combining a laparoscopic stage with thoracoscopic approach, as well as a cervical stage. Advantages include reduced postoperative pain, shorter hospital stay, faster recovery, and reduced complication rates. However, the presence of severe concomitant pathologies, such as grade III scoliosis, significantly complicates surgical intervention and requires careful anesthetic and surgical planning. Nevertheless, with a multidisciplinary approach, taking into account anesthetic support, adaptation of surgical stages to anatomical changes, and thoughtful postoperative management, it is possible to achieve a positive outcome even in complex clinical situations.
злоякісне новоутворення стравоходу; мініінвазивна езофагектомія за McKeown; кут Кобба; сколіоз ІІІ ступеня; однолегенева вентиляція
esophageal malignancy; minimally invasive McKeown esophagectomy; Cobb angle; scoliosis grade III; one-lung ventilation
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Shemmeri E., Wee J.O. Minimally Invasive Modified –McKeown Esophagectomy. Surgical Oncology Clinics of North America. 2024. URL: https://doi.org/10.1016/j.soc.2023.12.020.
- Usenko O., Sydiuk A., Klimas A., Sydiuk O. Postoperative anastomotic complications in patients with malignant tumors of the esophagus and esophageal gastric junction cancer. Світ медицини та біології. 2019. № 2(68). P. 135-141.
- Usenko O., Sidyuk A., Klimas A., Sydiuk O., Savenko G., Teslia O. Lung metastasis after pneumonectomy: Is there a place for surgery? Clinical Case Reports. 2021. V. 9. Р. e04954. doi: 10.1002/ccr3.4954.
- Sydiuk A., Sydiuk O. New formula for selection of an appropriate left-sided double-lumen tube size in thoracic anaesthesiology. Perioperative Care and Operating Room Management. 2021. Vol. 25. doi: 10.1016/j.pcorm.2021.100219.
- Savenko G.Yu., Sydiuk O.Ye. I. Lewis minimally invasive esophagectomy. Zaporozhye Medical Journal. 2022. Vol. 24(3). Р. 317-321. doi: 10.14739/2310-1210.2022.3.251586.
- Zhou J. et al. McKeown esophagectomy: robot-assisted versus conventional minimally invasive technique — systematic review and meta-analysis. Diseases of the Esophagus. 2022. URL: https://doi.org/10.1093/dote/doac011.
- van Workum F. et al. Totally minimally invasive esophagectomy versus hybrid minimally invasive esophagectomy: systematic review and meta-analysis. Diseases of the Esophagus. 2020. Vol. 33, no. 8. URL: https://doi.org/10.1093/dote/doaa021.
- Usenko O.Y. et al. Perioperative management of a patient with myasthenia gravis: a case report, treatment of myasthenic crisis and literature review. Emergency Medicine. 2025. Vol. 21, no. 2. P. 189-198. URL: https://doi.org/10.22141/2224-0586.21.2.2025.1854.
- Minimally invasive esophagectomy. The Multimedia Manual of Cardio-Thoracic Surgery. 2021. URL: https://doi.org/10.1510/mmcts.2021.020.
- Usenko O.Y. et al. Bronchoscopy in intensive care: to whom, when, why? (literature review). Emergency Medicine. 2025. Vol. 21, no. 3. P. 328-341. URL: https://doi.org/10.22141/2224-0586.21.3.2025.1876.
- Bonavina L. et al. Hybrid and total minimally invasive eso–phagectomy: how I do it. Journal of Thoracic Disease. 2017. Vol. 9, S8. P. 761-S772. URL: https://doi.org/10.21037/jtd.2017.06.55.
- Asti E. et al. Minimally invasive esophagectomy for Barrett’s adenocarcinoma. Translational Gastroenterology and Hepatology. 2018. Vol. 3. P. 77. URL: https://doi.org/10.21037/tgh.2018.09.16.
- Levy R.M. et al. Laparoscopic and Thoracoscopic Esophagectomy. Advances in Surgery. 2010. Vol. 44, no. 1. P. 101-116. URL: https://doi.org/10.1016/j.yasu.2010.05.002.
- Yu F. et al. Comparison of McKeown Minimally Invasive Esophagectomy vs sweet esophagectomy for esophageal squamous cell carcinoma: A retrospective study. Frontiers in Oncology. 2022. Vol. 12. URL: https://doi.org/10.3389/fonc.2022.1009315.
- Shanmugasundaram R. et al. Minimally invasive McKeown’s vs open oesophagectomy for cancer: A meta-analysis. European Journal of Surgical Oncology. 2019. Vol. 45, no. 6. P. 941-949. URL: https://doi.org/10.1016/j.ejso.2018.11.017.
- Makkad B. et al. Practice Advisory for Preoperative and Intraoperative Pain Management of Thoracic Surgical Patients: Part 1. Anesthesia & Analgesia. 2023. Publish Ahead of Print. URL: https://doi.org/10.1213/ane.0000000000006441.
- Shelley B., Licker M., Slinger P. Thoracic anaesthetic research: 90 years of sustained progress. British Journal of Anaesthesia. 2022. URL: https://doi.org/10.1016/j.bja.2022.10.034.
- Shoni M., Rodriguez G. Intraoperative Anesthetic Management of the Thoracic Patient. Thoracic Surgery Clinics. 2020. Vol. 30, no. 3. P. 279-291. URL: https://doi.org/10.1016/j.thorsurg.2020.04.011.
- Phelps J.R., Lizi H., Murphy B.A. Anesthesia for Global Ge–neral Thoracic Surgery. Thoracic Surgery Clinics. 2022. Vol. 32, no. 3. P. 307-315. URL: https://doi.org/10.1016/j.thorsurg.2022.04.001.
- Uhlig C. et al. Intraoperative mechanical ventilation practice in thoracic surgery patients and its association with postoperative pulmonary complications: results of a multicenter prospective observational study. BMC Anesthesiology. 2020. Vol. 20, no. 1. URL: https://doi.org/10.1186/s12871-020-01098-4.
- entrk M., Bingl E.S., Turhan . Should fluid management in thoracic surgery be goal directed? Current Opinion in Anaesthesio–logy. 2021. Vol. 35, no. 1. P. 89-95. URL: https://doi.org/10.1097/aco.0000000000001083.
- Huang F.-L., Yu S.-J. Esophageal cancer: Risk factors, gene–tic association, and treatment. Asian Journal of Surgery. 2018. Vol. 41, no. 3. P. 210-215. URL: https://doi.org/10.1016/j.asjsur.2016.10.005.
- Uhlenhopp D.J. et al. Epidemiology of esophageal cancer: update in global trends, etiology and risk factors. Clinical Journal of Gastroenterology. 2020. Vol. 13, no. 6. P. 1010-1021. URL: https://doi.org/10.1007/s12328-020-01237-x.
- Kitisin N. et al. Effect of Low-Dose Ketamine Infusion in the Intensive Care Unit on Postoperative Opioid Consumption and Traumatic Memories After Hospital Discharge: A Randomized Controlled Trial. Anesthesia & Analgesia. 2025. URL: https://doi.org/10.1213/ane.0000000000007419.
- Usenko O.Y. et al. Can the level of lactate and D-dimer isomers predict acute mesenteric ischemia? Pros and cons: a literature review. Emergency Medicine. 2025. Vol. 21, no. 4. P. 420-428. URL: https://doi.org/10.22141/2224-0586.21.4.2025.1891.